2021 was a busy year, for DEPTH and for researchers and communities worldwide. Here are some numbers that summarise our in-DEPTH work in 2021…
1
New research project, Routes: new ways to talk about Covid for better health. Focus on Gypsy Roma and Traveller communities, and migrant workers in precarious jobs. This participatory research is funded by the NIHR Public Health Policy Research Unit. The project responds to the Health and Security Agency need for urgent information on barriers and opportunities for improving health services relating to COVID-19 community prevention and response. Check out our brand-new webpage for more information.
137
Number of organisations and individuals contacted as part of our Routes project work, across mapping conversations, interviews, dialogue sessions and stakeholder conversations.
3
Major funders for our participatory DEPTH research: UK Government FCDO (ACCESS: Approaches in Complex and Challenging Environments for Sustainable SRHR), NIHR (This Sickle Cell Life) and UK Government NIHR/DHSC (Routes: new ways to talk about Covid for better health. Focus on Gypsy Roma and Traveller communities, and migrant workers in precarious jobs). Across these projects, we are working in dialogue with communities as well as with policymakers, researchers and advocates.
14
Points in our preliminary guidelines for equitable academic authorship in collaborative health research. We built on good-practice guidelines from the International Committee of Medical Journal Editors (ICMJE), the British Sociological Association (BSA) and Committee on Publication Ethics (COPE) to recognise the specific needs of authors in co-production contexts, including research conducted with non-academic collaborators. You can read our guidelines, for free, here.
2
Finalist nominations for the Royal College of Paediatrics and Child Health &Us ‘Voice Champion Award’. Dr Alicia Renedo and Dr Sam Miles were shortlisted for their work with children and young people, ‘championing their voices to inspire students and health workers at the London School of Hygiene & Tropical Medicine’. The nominations and shortlisting were run by young people. You can read more on our blog.
Total number of followers of our @DEPTH_LSHTM and our @ThisSCLife Twitter accounts. Check out our feeds out if you’re not signed up for daily updates, news articles and research findings.
90
Number of days we had to wind up a huge consortium project. ACCESS (Approaches in Complex and Challenging Environments for Sustainable SRHR) was axed without warning by the government in spring 2021. We nevertheless developed exciting outputs to share from our consortium work, available here. You can also read a summary of the project from our partners at IPPF (International Planned Parenthood Federation), here.
2
Strategy days to practice teamwork initiatives, discuss DEPTH priorities and plan our research strategy.
5
Total number of canine DEPTH team members. Gus and Ziggy are Sam and Laura’s puppies, while Bertie, Colin and Pepa are honorary doggie members!
Ziggy and Gus
We hope you enjoyed reading our ‘Year in 2021’. Watch this space for new developments in 2022…
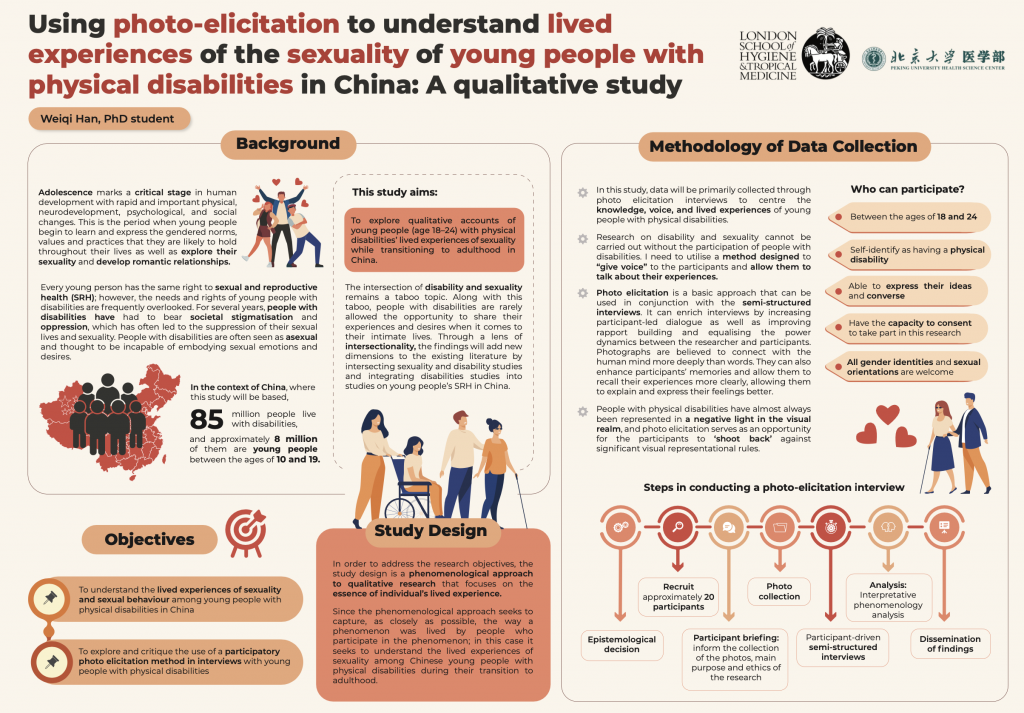
Our latest DEPTH blog comes from PhD researcher Weiqi Han, supervised by DEPTH Director Professor Cicely Marston, with LSHTM colleagues Dr Shaffa Hameed and Dr Emma Slaymaker. Weiqi has just wonbest poster at the 2021 Research Methods e-festival for her work on using photo-elicitation to understand the lived experiences of sexuality of young people with physical disabilities in China. Over to you, Weiqi…
‘I really enjoyed my time at the 2021 Research Methods e-festival last month, hosted by the National Centre for Research Methods and methods@manchester. Around 80 sessions were held over five days, with more than 130 speakers offering diverse perspectives on the festival’s theme: innovation, adaptation and evolution of the social sciences. The e-festival was brought together by a common interest in interdisciplinary approaches within and across the various social sciences. It was web based and was highly interactive. Attendees could join sessions via live video streams, take part in community discussion boards and network with other scholars.
I was so excited to win best poster at the festival. Currently, I am in the qualitative data collection stage of my doctoral work. I am honoured and grateful for this recognition, and I hope that it draws more attention to studies on the intersection of sexuality and disability.
For many years, people with disabilities have encountered societal stigmatisation and oppression, which often causes them to suppress their sexual lives and sexuality. People with disabilities are often seen as asexual and thought to be incapable of embodying sexual emotions and desires. The transition from adolescence to adulthood is a time of instability, experimentation and exploration in various areas of life, most importantly in relation to sexuality. In the context of China, where this study will be based, 85 million people live with disabilities, and approximately 8 million of them are young people between the ages of 10 and 19 years. Everyone has a right to sexual and reproductive health, and young people with disabilities should not be denied this inalienable right simply because of their disability.
The study seeks to explore young people (age 18–24) with physical disabilities’ qualitative accounts of their lived experiences of sexuality while transitioning to adulthood in China. Accordingly, a phenomenological approach to qualitative research will be utilised that focusses on the essence of the individuals’ lived experiences. Data will be primarily collected through photo elicitation interviews to centre the knowledge, voice, and lived experiences of young people with physical disabilities.
People with disabilities are rarely given the opportunity to share their experiences and desires about their sexuality and intimate lives. Research on disability and sexuality cannot be carried out without the participation of people with disabilities. People with physical disabilities have almost always been represented in a negative light in the visual realm. To enhance the participant-led understandings of experiences of sexuality and disability, I decided to utilise a method designed to ‘give a voice’ to the participants and allow them to talk about their experiences. Specifically, I will use photo elicitation in conjunction with semi-structured interviews to gain a ‘phenomenological sense’ of the importance and meanings that the content of the photos holds for the participants while allowing them to relate and share their issues, experiences and concerns.’
Weiqi’s work station with her cat, Mia, keeping watch.
Thank you for your guest blog Weiqi, and we look forward to learning more about your project in this historically under-researched field. Watch this space!
As always, comments are welcome on this blog. You can also contact Weiqi for more information on weiqi.han@lshtm.ac.uk.
New term, new research! We’re very excited to publish our latest article: ‘Reimagining authorship guidelines to promote equity in co-produced academic collaborations’, open access in Global Public Health. This piece brings together our thoughts on academic authorship from our recent ACCESS project on sexual and reproductive health and rights (SRHR) for marginalised populations, with our thinking on knowledge co-production from the project ‘This Sickle Cell Life’, a sociological study of young people’s experiences of paediatric to adult healthcare transitions
The call for papers for a special issue of Global Public Health on ‘(Re)imagining Research, Activism, and Rights at the Intersections of Sexuality, Health, and Social Justice’ offered us the perfect opportunity to crystallise some of the discussions we had and are still having as a research team about health co-production, academic research, authorship, and social justice. We take collaboration and engagement very seriously in DEPTH here at LSHTM, and felt that established authorship guidelines, while excellent benchmarks for ethical research and publication practices, aren’t always fit for purpose when it comes to co-produced work with different stakeholders. As we reflect in our Discussion:
There are numerous structural barriers to full collaboration that have an impact on authorship. The structural barriers to collaboration in general can be revealed in decisions about authorship – they are highlighted in who makes authorship decisions, and who benefits from them, and the structures and conventions that support and entrench inequities and devalue collaborative in favour of competitive working.
In light of these tricky contextual norms, we found numerous questions that needed unpacking: who is an author, and what do they contribute? When does a person’s place in the acknowledgements change to place on the author list, and when should it? How might we think more deeply about academic products and knowledge so that we do not inadvertently help supress voices that are already less heard? These voices are often less heard in academia because of the structures and customs of the academic system, so what impediments can we sidestep while acknowledging we still function within that system?
The result of our discussions is the article, which starts to explore how we might more explicitly pursue recognition of co-produced contributions to academic research. One way to hold ourselves and each other to account in equitable ways of working is through authorship guidelines, which we hope will prove useful as a jumping-off point for others engaged in collaborative work – especially with practitioners, activists, or non-academics, whose contributions and knowledges don’t always fit neatly into academic ‘boxes’. Having reflected on who tends to be disadvantaged by the current systems, we suggest that spending time thinking critically (and sometimes painfully) about these positions and relations can help to scaffold authorship norms that are fairer and more transparent.
You can read the whole piece here, free and open-access. But in this blog I wanted to highlight our authorship guidelines specifically. They are amended from existing excellent offerings of ICMJE and BSA, and move beyond them in that here we incorporate more explicit attention to different stakeholder contributions, and also to co-produced outputs. These are both themes that are long overdue more sustained reflection, and in an academic context of ever-increasing cross-disciplinary and cross-country collaboration and co-production with communities, we hope they prove useful for other researchers out there.
Take a look at our suggested authorship guidelines and see what you think – and reply to this post if you have suggestions for improvements or any other comments:
1. The nature of academic publication processes and authorship conventions should be explained to all partners so that the meaning of authorship and involvement is clear to all parties regardless of university affiliation or discipline.
2. The project research/writing team should list details of expected papers early in any sub-project, including expected authorship and author order (especially first author).
3. The rationale for authorship and author order should be transparent. All authors must make a substantive contribution to the intellectual content of the publication.
4. Non-academic project partners should be invited to co-author the work, with plans in place early on about how to handle suitable contributions. Level of input required must be discussed and agreed early on to ensure clarity on how authorship is allocated.
5. Contributors whose contribution does not in the final product meet the criteria for authorship should be named in the acknowledgements. Named individuals must be informed so that they can withdraw their name if they wish.
6. Where used, translators/interpreters must be named in the acknowledgements.
7. Lead author must draft the paper, with input from other authors, and be responsible for submitting the paper and making any revisions in response to referee comments. The lead author must not submit any paper without the agreement of the named authors.
8. All academic publications should contain a statement about the contribution of each named author.
9. The PI must approve submission of academic articles from the project and must be named as author if criteria for authorship are met.
10. Academic journal publication must be supplemented with publication of findings in other channels to ensure inclusive dissemination (e.g. tweets, policy document, media article, public workshop).
11. The particular needs of members of the team should be considered in arranging publication strategy (e.g. need to gain experience of lead authorship). However, any named author must fulfil the requirements for their authorship position.
12. Sole authorship will not generally be possible or desirable within the project because of the collaborative nature of the work and our recognition that knowledge is co-produced through these collaborative relationships.
13. Consider adding the consortium or project name to all work with numerous contributors who do not meet the criteria for authorship and listing key contributors to the paper in the acknowledgements.
14. In the event of any disagreements or confusion about authorship or author order, please refer to these guidelines within the writing team. If there is still confusion, please request assistance from the PI as the question may need to be referred for a wider discussion and/or the guidelines may need to be clarified.
In uncertain times, it was a real morale boost to receive some good news from the Royal College of Paediatrics and Child Health (RCPCH). The RCPCH ‘& Us’ team, who advocate for and involve children, young people and families in health services, recently told us that DEPTH researchers Dr Alicia Renedo and Dr Sam Miles from LSHTM were nominated for the RCPCH & Us Voice Champion Award.
The Voice Champion Award is a youth-led award recognising adults that go over and above their job role to work with RCPCH &Us to improve services with children, young people and families. The nominations were all anonymised and reviewed by young people from RCPCH &Us, who created criteria and a scoring system, then worked virtually together to review and discuss the fantastic nominations.
Alicia and Sam were not only thrilled to be nominated but also impressed by the youth-led nature of the nomination and award process. Putting young people at the heart of health services participation is key to how we work in DEPTH, so the RCPCH & Us Voice Champion Award feels like a real reflection of the values that we prioritise in DEPTH, too.
This Sickle Cell Life is an NIHR-funded research project that explores the voices and experiences of young people with sickle cell as they transition from paediatric to adulthood, and adult healthcare services.
Project Research Lead, Dr Renedo, says of the nomination:
“This was excellent news for the DEPTH team. We admire the work done by RCPCH &US, and they are a role model for participation, so coming from them, this nomination felt very special.”
Project Principal Investigator and DEPTH Group Director Prof Cicely Marston said:
“I’m so delighted to see Alicia and Sam recognised in this way. They work really hard to make sure our participatory work is inclusive and their work with young people on this project has been brilliant.”
We feel very honoured to be nominated, and thank all of our collaborators and colleagues for their role in making This Sickle Cell Life happen. You can read an ‘Evidence’ brief of This Sickle Cell Life by NIHR here.
Some of the This Sickle Cell Life collaborators (Top row L-R: Patrick Ojeer, Ganesh Sathyamoorthy, Sam Miles, Nordia Willis, Alicia Renedo, Andrea Leigh. Bottom row L-R: Cicely Marston, John James, Siann Millanaise. Photo: Anne Koerber)
This interview focuses on working with young people in a tricky year when it comes to participation. We asked Emma how RCPCH &Us have managed to carry on with engagement activities since Covid…
Adapting and engaging in a pandemic
Emma: We had to look at all of our projects and decide which ones are appropriate to carry on, because we had some that were about very sensitive topics that in-person would have been challenging, and would have needed a lot of support and aftercare – for example complex respiratory illnesses. We looked at those and thought, you know, what, there’s a pandemic going on, which includes respiratory illness, now’s not the time to be phoning people up or talking to them and saying, ‘what do you think about this?’ and ‘what you think about that?’ First we did a wellbeing assessment on our workstreams and agreed which ones we were going to park for a bit, based on a welfare context. Then we spoke about what the missing gap in provision might be, because everybody is going to suddenly do everything the same and we don’t want to duplicate. We actually didn’t go as quickly as some of the other organisations to put out loads of new children and young people-focused information about COVID. What we did was pull together existing information on COVID and put it into a place that was easy and clear for families, parents and children and young people to see.
We wanted to give children and young people a meaningful role and we had to be creative
One of the things that we wanted to do was give children and young people a meaningful role. We asked: what are the gaps? Something that came up from paediatricians was that they were really worried that children and young people wouldn’t be going to their regular appointments anymore, so could we create a child health diaryfor them? So we did, and that’s still getting downloaded now, which is really cool. It’s something a bit more creative for them to write down their questions or things that have happened that are good. A doctor came to us and said ‘we want to thank our children and young people for taking part in the covid effort and not coming in and not playing outside, so can you create an E-card?’ So we created e-cards for thank you and birthdays, and last month 5,000 of those were viewed.
We picked up on children’s and young people’s concerns
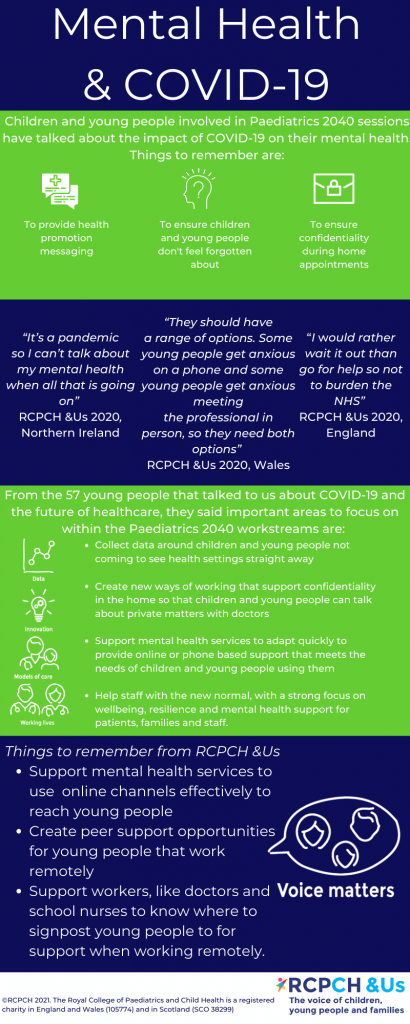
As time went on we worked with lots of other groups, virtually. Lots of Teams, Zooms, and all that kind of stuff, to find out: what’s happened for you with health during COVID? What are your appointments like and what are you missing? What’s the information like? We picked up concerns from children and young people about the fact that COVID information wasn’t targeted at them. It was for adults. It also wasn’t giving a positive message about children and young people, so they were seen as the problem rather than part of the solution. There were also significant gaps forming around mental health support. That led us into a couple of new projects focused on COVID, but specifically from children and young people’s points of view. One was about mental health in a crisis, where we wanted to children and young people to tell us where they’re getting their mental health support and where are the gaps. Another one is working with young people to try and get a press conference for young people, because they’re not allowed to ask questions at the government press conferences, you have to be over 18 – excluding a whole group from having their questions heard or having a role. So we’ve been working with other charities to call for a press conference to answer questions from children and young people.
We got young people involved in reviewing evidence on patient experience of COVID
Finally, we realised that there were thousands of studies being done on COVID. The RCPCH had clinicians coming together to review which studies were being published on children and COVID, which got me thinking that actually there was also thousands of studies being published of what young people had said. Lots of charities were asking their children and young people about the impact of the pandemic, and then publishing the results. And we just wanted to give young people a chance to also do what the adults are doing: so if doctors can review scientific journals about COVID, young people can review a patient experience of COVID. We pulled together a group of a small group of young people and over 12 weeks, invited them to look at about 20 different published studies of around 60,000 children and young people’s voices, say, from cancer patients, mental health experiences of young people, children and young people or young carers, across the UK.
And they did what we do in our world – they conducted some thematic analysis, they explored the key trends, they developed them, they then created eight different topics that came up, and they slotted in the data, with a ‘for’ and ‘against’ for each topic. Topics included things like mental health and family dynamics, employment, education. They wanted to make it make a difference to the NHS, and the NHS at the moment are writing recovery plans on how to how to restart the NHS. So they’ve boiled all of that work down and they volunteered over 100 hours doing this project over about three and a half months. They’ve turned the three priorities they have developed for the NHS into posters. The posters include the priority, the problem, the solution, the impact, a quote and some stats. Since launching, the recovery plan priorities have had about 28,000 Twitter impressions. You can read more about the COVID Book Club findings online.
The work has elevated the voice of children and young people – and made people understand they have a lot to say
Emma: We also hosted a debate with doctors about whether paediatricians should be thinking holistically or medically during COVID, because for children and young people, it’s about their mental health as well. That project just feels so different from what we’ve done before. We had to really think through safeguarding and wellbeing, so we didn’t overwhelm the young people who led it. This project very much felt like we were actually paralleling something that was going on in the academic part of the college, and doing the exact same thing, but for children and young people, which felt very different. It has elevated children and young people’s ability, both in the college and in the sector. And it’s really made people understand that they have got a lot to say, and they understand what’s going on, and have a lot to offer.
So on the whole, we’ve managed to find a way or find a tool or find an approach that makes it fun and entertaining and interesting and focused on them rather than the topic sometimes.
The good thing about having to change our work is that we’ve been more connected to RCPCH wider internal projects. The benefit of voice has been seen in a different way. And for us, we had to take that opportunity and run with it – we’ve had 200 new children and young people involved during the COVID pandemic, who have between them completed over 330 hours of volunteering.
Voices are being heard and the professionals are engaging more
Emma: We give advice to people that are starting out on a project or want to talk about PPI [patient & public involvement] and I’ve had so many more requests over the last three months for people that want that advice. And I think it’s because children and young people’s voice is now seen differently. They’re really seen as being integral. There’s so much further we could go, there’s a million other things we could be doing that are even more innovative and creative, and increasing their reach, but you’ve got to start somewhere.
Barriers to participation – too much time online but also digital exclusion
Emma: There’s different barriers and challenges according to which audience you’re coming from. For children and young people, one of the challenges that they’ve said to us is that it’s really overwhelming that everything is online. We’ve really got to understand that because whilst we think we’re doing something fun and exciting, and it’s online for an hour, they’ve already had school online, for some of them health appointments online, mental health appointments, and counseling online. They’ve had zoom calls with friends and family, they’ve tried to keep fit online. And then we’re coming at them with another online thing. Another challenge for them might be: maybe I haven’t got somewhere confidential and private to do online stuff where people aren’t listening in. Or maybe I haven’t got a good device. So we’ve really looked at the challenge and been as inclusive as possible. You can join our online sessions on phone, you can do it on WhatsApp, you can join via video, you can have no video. You can use the chat, or you don’t have to use the chat, you can do it by email if that’s better – it’s all your choice. For us it’s a challenge because we’re having to run four or five different tech options for a one-hour session. But it’s about understanding that not all children and young people want to be on video, not all children and young people have got a device that lets them Zoom. Maybe all they’ve got is a landline, which means they can phone in.
The challenge for participation and engagement is don’t get complacent and think that your games and activities can all work with everyone seeing everything, because they can’t. It’s about inclusion. And that comes from children and young people saying: I might be sharing my laptop with five other people in my house, so I can’t use Teams at the same time, but I will phone in because I’ve got a mobile. We’ve had to really think it through. Another challenge is always remembering whatever you’re talking to children and young people about might be overheard. So don’t put them in positions that makes them disclose stuff that actually might not work well in their family environment. We’ve worked hard to create safe spaces, and to work with each group that we’re talking to, to make sure we understand what their space is like at that moment. Because you can’t start a conversation about money and poverty, when their parents are listening and they might feel that they’re being judged or that the young person feels like they’re judging their parents or living environment.
How can we make it fun? How can we make it inclusive?
Another challenge has been how we can make it feel fun. If you’re using devices for presentations, or for school, we don’t want to be like school on your computer. In the back of our heads we’re always thinking let’s not overwhelm our children and young people, they don’t have to come to the project if stuff’s going on. So we’ve really been conscious about trying to understand what people might be going through. And then to think about things like don’t drink or eat when you’re on camera, because not everyone has got enough food in their house. You would do that in the meeting room, but if we were in the meeting room, we would have given them food and drink. Whereas for us on camera, we’re being really careful about stuff like that. So I think that there’s some challenges. The one that we’re looking at now is where we would normally do community outreach to reach people who aren’t connected to any projects. That will be a challenge and we need to think about how best to reach out to that cohort. But no challenge means that it’s the end and we’re not there yet! It just means that I need to think harder about how I’m going to get past it.
I knew the COVID studies review would give young people a platform that they’ve never had before. But how can you possibly do that safely? If I was in the room, I’m able to see their visual cues, I’m able to unpack things over lunch, I’m able to stop the session and do something entirely different. I spoke to a friend who’s a youth worker and she said: ask the young people, they’ll tell you what works for them, so we did, and they knew all the answers and helped shape the project throughout. In the end they decided that we couldn’t do all of the studies. We found 33 but they said that they could only manage a certain number but that’s cool. At every stage I just kept checking in with them. They will tell us what works for them. It’s co production even in that sense.
What tools can we use for remote working with children and young people?
The first thing I would have to say for anyone about to do is go and talk to your information governance manager. Because whatever you think might be able to be used might not be able to be used for lots of different reasons. One thing we used is Trello , because the young people said for the COVID studies review they wanted somewhere where they could collaborate on documents, but we can’t use Google Docs because of a GDPR issue. I’ve never used anything like that before with young people. It’s so good. They could ask questions and comment on each other’s documents. But they could also see really clearly what was happening at what stage and what they could add to if they had a bit more time. I’ve been trying to find a voting app online, because that is key to so many of our projects, to be able to anonymously prioritise five or six different things. And Menti allows you to do that. You don’t have to put any personal data in, you just get given a code. And then they’ve got lots of different voting tools that you can use. Having a virtual whiteboard is really important as well, like JamBoard. But going back to inclusivity, if we’re using JamBoard, and I’ve got two people that phoned in, I will take a screen grab of it and then WhatsApp it to them so they can see it building. And it’s keeping that in mind as well, to make sure that you’re not inadvertently excluding someone because they haven’t got the same software in front of them.
Overall, I think we keep adapting, learning and changing to the meet the needs of children and young people engaging with us through the pandemic, as we learn new digital tools or approaches and learn from the group. It’s been an opportunity to really relearn everything you have always done and to reflect, update and adapt which has been hard at times but so rewarding when you see the outputs and outcomes.
Attendees at the participatory dissemination event for This Sickle Cell Life with DEPTH at LSHTM and RCPCH’s &Us (Photo: Anne Koerber)
Contacts
To find out more about the RCPCH &Us programme or to access their free resources and support go to www.rcpch.ac.uk/and_us or contact and_us@rcpch.ac.uk, and follow them on twitter @RCPCH_and_Us.
You can read about the RCPCH & Us collaboration with LSHTM on ‘This Sickle Cell Life’ here.
We began by asking Emma to explain her role, and how she and her team approach child health and engagement.
Part 1: How do we engage with children and young people and amplify their voices?
Improving child health is more than just paediatrics
Emma: The Royal College of Paediatrics and Child Health (RCPCH) is a charity, but as a Medical Royal College, it helps to support the specialism of Paediatrics. We’re slightly different to other Royal Colleges because we are the Royal College of Paediatrics and Child Health, rather than the Royal College of paediatricians. So it means we can get involved in the whole child health agenda, which is obviously much bigger than just paediatrics. The RCPCH &Us programme is the network for children, young people and families to help inform and influence all of the work of the College. It gives them a place to have their voice and space to say what’s going on for them and what could be done to improve child health services. Our approach is to get them involved in that – it’s not just somewhere to chat, it’s somewhere to actually get involved in and progress social action. For us it’s like a network approach where we try to get as many children and young people and families involved across the whole of the UK at all ages. This year, our youngest person involved is aged four, and we go up to age 25.
We focus on children and young people’s voice and having them involved as volunteers or project members or giving views, but we also recognise that sometimes we will need to involve their advocates as well, whether that’s parents or carers. So we do ad-hoc work with parents and carers, but our primary focus is making sure that children and young people can get involved in the work the college is doing. We also ask what might be some of the challenges in child health, that they’re keen to explore and do something about with us?
People ask what children and young people think about something… We turn the questions into games and activities and take them out on the road
Emma: Our approach is a bit different to most places. At RCPCH &Us, we work in three different workstreams. One is our roadshows and consultations. We get questions from loads of different people about what do children and young people think about something – for example at the moment I’ve got questions on what do young people think about virtual health appointments, and what do children young people think about mental health experiences? What do children and young people think about how their data is used? There’s lots of different questions that come into us. We’ll turn these questions into a set of games and activities and take them out on the road, so that we can go and speak to as many children and young people as possible in as many different areas as possible, with as many different experiences as possible. It’s about us being out there with them, rather than expecting them to fill out a survey or a questionnaire or attend something with people that they don’t know. Our roadshows might operate through schools or youth centers or playgroups or outreach. Or we might speak to children in care groups and carers, or speak to children and young people who are patients: we’ll speak to them outside their outpatient appointments, when they wait to see their clinician, or they might be inpatients.
We bring young people together for day-long ‘challenges’ or for long-term projects
The next approach is challenges. These are ‘tasters’, because children and young people don’t necessarily want to sign away their lives to a project for three years, they might want to just see what it’s like. We’ll bring them together for a project day, where they’ll come in not really knowing that much, and then learn all about a topic, they work with data, and come up with solutions and then present it at the end of the day. This is a bit like the project that we did with you at LSHTM last year – This Sickle Cell Life.
The final approach for us is long term projects focusing on a specific area, with children and young people signing up to join that project team.
Developing workshops in the participatory dissemination event for This Sickle Cell Life (Photo: Anne Koerber)
Children and young people can participate in a way that works for them
Across our approaches, you could be a young person or child that just wants to tell us something in a conversation, that’s perfect. Or maybe you want to try something you want to do a challenge or maybe you want to do a project, but you don’t need to do all three; children and young people can come in and out as it fits for them. We really want to make it an opportunity for them that they feel is meaningful, and that fits their life rather than fits my nine-to-five work life. It includes lots of weekends and evenings, and lots of doing things in lots of different ways. But for us, that’s important because it means that we get more children and young people involved who might not have been involved before, across different ages and backgrounds.
The other bit that is different is the way that we approach diversity. So we also make sure that any project we’re doing has children and people from three different groups. One is universal, so they’re all just children or young people, because that’s who they are. Then we have a group where they’ve got specific experiences that might change the dynamic for them, for example they’re young carers, or they’re Gypsy travelers, or something that binds them together with an identity. The third group is specialists, who have the health condition, for example asthma. That explains the way that we try to deliver our work by bringing together all three groups to have a full set of views, ideas and experiences.
How do adults respond to your approach, and the way you centre children and young people?
You’ve always got people that are your allies and they’re brilliant for amplifying what’s going on. You can send them something and explain it to them and you know they’re going to get it straightaway and get it out. And then you’ve got the middle group who know that it’s important, but maybe feel stretched – overwhelmed by their work or their role. But when you can engage them in a conversation with an adult, or an organisation or a particular group of people you can see that they get it and they want to do more, but maybe the time is just not right. Those ones stay in touch, and they will get there. Then you have the people that just don’t get it at all. Either they fundamentally don’t want to get it, because they don’t think it should be happening – you’ll have people saying, ‘but why, it’s not [children and young people’s] role to say that we know what we’re doing’. Or they don’t get it because actually they’re at a point of crisis themselves, maybe in their role or their organization where it’s entirely the wrong time.
We just have to really understand that we’re going to have all of those groups, and they’re all important. They all have a role to play in what we’re doing, but the way we approach them will need to be different. So the information we give to allies and the people that ‘get’ it is what children and young people have said, and can you do something with it? Yes. The middle group, we see how we can show them the benefits of what children and young people are saying and then how it will actually support their work. For the ones that fundamentally don’t get it, we tend to talk about the legislation: there’s a statutory duty to do this, it isn’t something that I’ve just made up. It’s really important when you do engagement work that you’re aware that everybody has a different motivation as to how it will land with them, and why they might be interested. But you can learn from them and work to give them what they need. Sometimes it’s challenging but I just see it as an opportunity to share information in a different way. I have to just try harder to make sure that that it meets what they need.
I think you have to be an eternal optimist in engagement work, because everyone’s different, everyone learns in a different way, everyone participates in a different way. It’s all part of a process.
Attendees at the participatory dissemination event for This Sickle Cell Life (Photo: Anne Koerber)
Thanks for your time Emma. Look out for Part 2 of this Q&A next month!
Contacts
To find out more about the RCPCH &Us programme or to access their free resources and support go to www.rcpch.ac.uk/and_us or contact and_us@rcpch.ac.uk and follow them on Twitter @RCPCH_and_Us.
You can read about the RCPCH & Us collaboration with LSHTM on ‘This Sickle Cell Life’ here.
The new research partners within the ACCESS SRHR (sexual and reproductive health and rights) consortium. We are looking forward to working with colleagues at LSHTM Uganda and HERD International, Nepal.
The number of citations of our piece in The Lancet, Community participation is crucial in a pandemic. In it, we lay out steps governments and health bodies must take to ensure citizen participation.
The number of words in our final NIHR report, This Sickle Cell Life. You can learn more about the findings from our project here.
The number of sickle cell patient and carer experts with whom we co-produced This Sickle Cell Life. We recently collaborated with them to present study findings to London NHS Trusts.
The number of new followers to our @DEPTH_LSHTM and our @ThisSCLife Twitter accounts. Check them out if you’re not signed up for daily updates, news articles and research findings.
The number of hits on our tweets in 2020 from our DEPTH Twitter feed. If you don’t follow us already, now’s your chance!
New year, new blog post! For our latest piece, DEPTH researcher Dr Sam Miles reflects on the journey from PhD to first academic job, and offers some advice to ECRs (early-career researchers) pursuing careers in academia. This blog has been adapted from The Royal Geographical Society ‘Postgraduate Life‘ Series, which you can find here.
I was recently invited to write a guest blog for the Royal Geographical Society about my journey to my first academic job. I don’t have all the answers – in the piece below I reflect on exactly why this might be, and my concerns probably resonate with many of you – but I do have some ideas. Many of these came about after discussions with former students, current colleagues and other early-career researchers (ECRs) in the field, and notes of my own taken over the years.
It’s not as simple as a tick-list, though I cannot tell you how much I wish it were. I just hope that these ideas can be helpful to social science students here at LSHTM and in the wider job market applying for postdoctoral or lecturer posts. I was asked to write the kind of blog post I wish I’d read when I was starting to job hunt; with that in mind, here goes.
It’s one of those truisms that finding an academic job is hard. And it really is – it feels somehow unlike finding any other kind of job, and the specific knowledge around academic job hiring processes is something you’re also somehow expected to know, maybe by osmosis. It’s no wonder Imposter Syndrome strikes so many of us. Take for example academic CVs, where longer is better. It goes against every fibre of my being to go over the 2 pages I was always told is the maximum you should fill. Even the listing of education/jobs/experience is differently ordered in an academic CV to CVs in every other job in the world. Job adverts themselves can be confusing in terms of terminology and contract type, or arcane or unclear working conditions, or freighted with acronyms without explanations. On top of this, salary, contract length and expectations of entry-level posts can be vague, missing or intimidating.
It all results in a task that feels unclear and applications that can feel rather uncertain. Usually, that’s through no fault of your own (as evidenced when you’re several applications in, facing radio silence from each institution. Are you even doing it right?) Obviously, the offer of an actual job would answer that question, but academic posts are so competitive that your empty inbox may be more of a testament to a stricken job market than your own application – and the COVID-19 pandemic has made a precarious market even worse. You will often be rejected without any feedback from the hiring institution. The standard response to requests for feedback is that feedback is only feasible at shortlist stage, but it is invariably difficulty to get to shortlist and interview if you don’t gain feedback on what you need to finesse! In the absence of clear direction from institutions, you may need to utilise a few different approaches. I’ll lay out some that I used.
Here’s what my own journey looked like: In the final year of my PhD, I applied to several lectureships. The applications I submitted were for posts that normally required a PhD, completed or near-completion. I took this to mean that they were open to nearly-there or newly-minted PhDs as much as anyone else, but have since recognised that the field of candidates is routinely so huge that many will have progressed a long way beyond this milestone. From asking more established colleagues at my institution, talking with early-career-researchers at a conference that spring, and looking out for the hiring announcements of successful candidates (people increasingly share job successes on Twitter), I realised the reality was that new PhD finishers rarely get these jobs. The market is crowded with brilliant and highly-qualified candidates. Vacancies are limited (and by some accounts, dwindling further).
It is now much more common for PhD finishers to work on one or several assistantships or postdoctoral posts before lectureships become a possibility. Even then, that post is often fixed term.
During my own job hunt, a Research Fellow post at the London School of Hygiene & Tropical Medicine (LSHTM) caught my eye. It required a PhD in public health or related discipline, including social sciences. Alongside my own research covering some (but certainty not all) elements of sexual health via a PhD researching the mapping of queer male relationships on location-based dating apps, I made sure I researched reproductive health, which was the other component of the post and an area where I was less experienced. The specification emphasised qualitative methods, which matched my experience, and co-produced research outcomes with communities. My doctoral research was participant-centred and I had been reflecting on making a safe space for sensitive topic discussions, but I wanted to develop this more in future work. The LSHTM post would specifically engage participatory research, so I took my knowledge of participatory action research (PAR) from my own work and brought myself up to speed on co-production and PPI (patient/public involvement) in health.
I revised (and revised, and revised) my academic CV, highlighting teaching experience as well as research outputs to date. I wrote a targeted cover letter which addressed each of the candidate specification requirements listed in their ‘essential’ list for the vacancy. I addressed each criterion only briefly, keeping the letter to the point, but then noted down longer answers to consider for a potential interview stage. The hiring panel requested academic and non-academic writing samples, so I included a published article but also a blog I had written about the Pulse nightclub shooting in Florida and its impact on LGBTQ space. I was shortlisted for interview(!) and prepared obsessively. I read articles, chapters and media pieces from the hiring team, and took them up on their invitation to produce a slideshow to present in the job interview. I tried to make sure I could highlight the ways in which my research experience matched their goals and I matched up every item in the person specification to a demonstrable activity, role or expertise. This is so key:
You need to show how you fulfil each and every ‘essential’ criteria to progress to shortlist. If you cannot show this, or don’t effectively communicate how you show this, your hiring panel will not be able to ‘get to’ other elements of your application that are lower ranking in priority.
And… I got the job! It was only a one-year contract, but with hopes of renewing this pending funding. That happened at the end of year one, and then again six months later, and again a few months later. Three years later, and I’m still hanging on. We are now embarking on a very exciting project, after which point I will again need to think about new grants, funding and tenure.
This brings me to precarity. One thing I was asked to reflect on in my blog post was worries I had when applying for academic posts. To be honest, it’s not a past tense concern: I’m funded for now, but then I’ll need to generate grant money for future posts. What started as a temporary position became less precarious, but I’ve yet to secure a permanent position, and know strikingly few ECRs who have managed it. Over half of all UK lecturers are now on fixed term contracts. I worked for several cash-strapped NGOs before my PhD and yet have never experienced precarity like I see in academia.
It’s not a personal failing of mine – nor of my colleagues, my line manager or even my Faculty. It’s the predictable result of the neoliberalisation of universities. ECRs are good value and high output, and the incredibly high requirements of REF and general institutional reputation require in turn workers who can relentlessly publish lots of high-quality, peer-reviewed research. In this context, the idea of ‘slow’ co-production in research sadly becomes a luxury, even as my colleagues and I have shown its value.
Find academic jobs advertised on jobs.ac.uk and Times Higher. Jobs.ac.uk is better in my view because it allows tighter filtering by salary level, city and discipline. You can also ask it to direct new job alerts straight to your inbox.
Twitter is an incredibly useful tool, not just for academic networking, but for getting to know an institution and who works there (many staff now have Twitter profiles – DEPTH even has one). It’s also useful to catch job alerts from departments in case you’ve missed them on your job hunt.
Write a blog. It’s a tip I bet you’ve heard before and probably rolled your eyes at, but it’s true. Writing your own blog as a PhD student is invaluable. I may not keep up a regular blogging schedule, but writing a blog, especially at PhD level, has been useful for thinking ideas through, for connecting with other people online, for publicising my work. My hiring committee told me that they read writing samples closely to check that candidates can articulate ideas, and they judge generalist and academic writing equally. Writing a blog allows hirers to witness your skills already in action as a form of public engagement.
My PhD supervisor, who was relatively early into their academic career themselves, was a source of invaluable advice, and I would definitely recommend asking to speak with your supervisor in your final year about your job application plans. Ask to do this separately from your normal supervision slot if that’s what it takes to really get your head in the job hunting zone. Talking your plans over with a supervisor is doubly useful if you have sent them your CV in advance for them to review or comment on.
Your supervisor has been in your position themselves, and so their advice should be invaluable, but I also know that many supervisors haven’t been on the job market in years. Even if they have, the reality of today’s academic job market may be totally different from their understanding. They also may not have time to help you with cover letters or CVs. If this is your experience, ask around to see if another staff member – perhaps your head of department or research lead – would be willing to look over your application materials.
Find your university careers service and book a CV appointment. Be clear when booking that you are applying for academic jobs and need guidance on an academic CV and cover letter – the advisor is unlikely to be specialist in that area but at least you’re giving them the chance to check up on the conventions in order to offer you tailored help. In my case at QMUL they didn’t have anyone relevant in-house but hired a specialist for PhD students as and when required – the consultant was excellent, and free for students.
Take some precious days away from thesis write-up to rehearse how you can show your interview panel specifically how you are the best matched candidate for the role. I’m always surprised that most people I know don’t do this, which surprises me (they also tend not to rehearse conference presentations either – horses for courses, I guess). It seems obvious that the rhythms and flow of public speaking aren’t perfected on your first run through, and that goes doubly for a speech or presentation. Do I hate it? Yes. Do I force myself to set time aside for the activity anyway so that when it comes to the real thing ‘out there’ my flow mitigates my wobbly voice or mumbling? Absolutely!
When universities hire a candidate for a post, they need to fulfil these criteria to be shortlisted and need to demonstrate their fulfilment of these criteria again in interview, so taking time to really read and think about how you match to these criteria is crucial. Think about it: you need to minimise their labour in matching up what they are looking for when it comes to interviewing their candidates. You need to prepare some of this work for them, so they aren’t having to find ways to invite you to show how you match up – because you’ve already laid it out concisely and persuasively, on the page and in person. Good luck!
For our latest DEPTH blog we asked LSHTM researcher Kimberley Popple to share her thoughts on NGO-academic collaborations as someone who has recently moved from the former to the latter. Thank you for your insights Kimberley – lots of food for thought!
Back in January this year I made the move from practitioner in the NGO world to becoming a researcher in the academic sector. I wanted to combine the skills I had developed in Public Health research with my knowledge and experience of programme implementation in the field. It seemed to me that there were obvious synergies and opportunities for practitioners and academics to work together to improve global health. Certainly, from my own experience, the projects that I worked on could have benefited from drawing on people with specialist skillsets in data collection and analysis and with the time to conduct literature reviews, produce evidence maps, and test the change pathways that many of the programmes were built upon.
Before moving into academia, I worked on a large portfolio of grants in Sierra Leone as part of the Ebola response. Most of the data we collected was used solely for routine monitoring and evaluation of interventions at the project-level. Its purpose was to track progress against set indicators and to report on spending to funders. As a result, collecting data that could be easily quantified was prioritised, and quantitative data was assumed by funders to show a greater impact than qualitative data. Further, qualitative data tends to fall within the remit of the accountability teams – it is used and relied upon but not as an indicator of impact. In the Sierra Leone scenario, success of an intervention was often measured by a high number of medical consultations or a large number of attendees at a meeting, rather than focusing on data related to quality of services or patient satisfaction. I remember one example of a gender-based violence (GBV) project in Freetown which was categorised by the funder as “underperforming” as the target number of survivors had not been reached. The fact that that the women who had been reached had received high quality support across the GBV spectrum of services was seemingly less valued.
In Uganda, I worked on a maternal health project which introduced a client-exit survey for women to participate in at the hospital after receiving maternity care. However, the survey was administered by NGO staff who were working with the marginalised populations, and in close proximity to the medical staff who had provided their care. There was little recognition of the power imbalance between interviewer and interviewee or the desirability bias that might be present as a result of the women’s fear of negative repercussions from medical staff.
Evaluations were often seen as a tick-box exercise for donors and their design was fairly rudimentary. By the time the evaluation report was written, the programme had already moved onto the next phase to align with strict funding cycles. This left little room to reflect on lessons learned and engage in a process of iterative programme design. A recent systematic review has highlighted the lack of evaluations conducted on epidemic responses in humanitarian and low-income settings, with only one tenth of responses evaluated and with large gaps in quality, content and coverage of evaluations, limiting the ability to improve future responses.
Over recent years, the international development sector has intensified its focus on evidence-based programming and evaluation. Many NGOs have increased their research capacity with dedicated departments and research staff (for example Airbel Impact Lab at International Rescue Committee, and the Response Innovation Lab at Save the Children), giving them the expertise and space to test out new formats for implementation, and to ensure programming is based on the latest evidence of what works.
New funding streams have emerged for research in the humanitarian field, such as Elrha’sR2HC programme, and there is donor pressure to evidence learning and use data for decision-making. Donors like the UK government’s Foreign, Commonwealth & Development Office (FCDO, formerly DFID) have developed more in-depth guidance on how to develop and use evaluation frameworks to measure impact and ensure accountability, with requests to include qualitative indicators in logframes.
What can academia bring to the table?
So, is there still a role for academics to play in supporting the work of NGOs? I believe there can be, particularly in the evaluation of complex interventions. Universities train public health professionals who often go on to work in the NGO sector. Expert knowledge of process and outcome evaluations can be drawn upon to test change pathways in Theories of Change. Systematic reviews can be performed by academics with fewer time and funding constraints, reducing the need to reinvent the wheel every time to search for the latest evidence. As academics, we can add our voice to campaigns as advocates of change. And the humanitarian health sector can harness specific skill sets in conducting clinical trials and in disease modelling. My sense is that as both sectors continue to develop and evolve, it will be important to continue to reflect on the value of academic-NGO partnerships for global health.
Self-testing swab. Photo credit: Anne Koerber, LSHTM.
The COVID-19 pandemic is requiring home-testing in large numbers, and this process raises questions about the ethics of informed consent. In our latest blog, DEPTH member Dr Catherine McGowan reflects on a route to informed consent and suggests how governments, healthcare groups and institutions can maintain informed consent in a time of crisis.
A key step in any research project involving human participants is gaining informed consent. COVID-19 has disrupted research work around the world, and it will continue to do so for many more months. In this ever-changing pandemic environment, important research must continue. However, this work still requires researchers to think carefully about how best to obtain consent remotely.
Photo credit: IEEE Spectrum
Researchers carrying out various population surveys are sending COVID-19 tests by post and encouraging people to self-test. Self-testing kits are a good example of a process that reminds us of the need to think about consent. Research participants must provide informed consent to participate in research, particularly when it comes to population surveys involving biological sample collection. Information governance in the European Union and the UK has changed considerably with the implementation of the General Data Protection Regulation (GDPR), which does not allow for presumed consent in most cases – so when it comes to a process like home testing, for example, the data gathered cannot legally be collected or processed without gaining explicit consent from research participants.
In 2017 we carried out antibody testing amongst non-Ebola infected healthcare workers (HCWs) who had returned from West Africa following the 2014/16 Ebola outbreak. We posted test kits to HCWs throughout the UK and the Republic of Ireland, with samples returned via post. When it came to getting informed consent, face to face consent was not feasible, we could not waive consent and nor did we feel comfortable presuming consent. In the interests of best practice we also wanted to make sure that participants had all of the information they needed in order to consent fully – and be able to reach us, the project PIs, with any questions they might have. Ultimately, we decided to recruit participants via email but first they were asked to work their way through the consent materials electronically, and to explicitly indicate their consent. Once participants had consented they were asked to complete a short questionnaire and to provide their postal address so that we could send out the test kits. At the conclusion of the study we emailed participants to let them know the results of their antibody test and included a link to a survey asking about their experience of consent. Our findings, as well as a description of the design of the consent process is described in our paper which you can read for free in Journal of Public Ethics. We asked participants how much of the consent material they read, how informed they felt and if they preferred online to traditional face-to-face consent.
The results were very interesting: Participants indicated a high level of engagement with the consent materials, with 67% reporting having read all and a further 20% having read ‘most’ of the materials. All participants indicated feeling completely (78%) or mostly (22%) informed about the purpose, methods and intended uses of the research, as well as what participation was required and what risks were involved. Overall, participants reported an overwhelming preference for online consent. Their longer free-text responses suggested that they were predominantly attracted to the convenience of online consent, including the leisure to read the consent materials several times, and the ability to engage in the consent process at a convenient time/place. Free text responses also supported online consent for our survey, but participants indicated that were the study more complex or were it a clinical trial they would prefer to have a face-to-face element.
Self-testing kit. Photo: Anne Koerber, LSHTM.
Obtaining consent in lockdown
What can this study tell us about the research based on COVID-19 home-testing that is happening now? Well, it is our hope that as researchers aim to continue their work online, they give careful thought to what informed consent is in the current circumstances. Our paper describes how to obtain informed consent electronically and in a way that we have found to be acceptable amongst our research participants, but this might not be appropriate in all cases.
We also hope that Public Health England puts in place a robust framework for the pandemic to ensure adequate consent is still sought and obtained for any research. It is in times of crisis that abuses may be allowed to happen. Even with the best intentions, researchers may act expediently and may overlook best practice in their hurry to conduct the research and obtain results. In disaster settings, corner-cutting in ethical research practices are more likely, but this is also when participants are most vulnerable and may feel less able to challenge research practices that feel inappropriate. Our own study has shown that there are easy and acceptable solutions for obtaining informed consent. We hope that researchers currently developing population surveys using self-testing methods will give some thought to developing acceptable solutions to obtaining informed consent. We must continue research activities without forgetting our professional, ethical, and legal obligations to those who make our work possible.
Photo copyright: Catherine R. McGowan. Photo consent from healthcare worker.