by Dr Farouk Garba, Ahmadu Bello University Teaching Hospital, Nigeria
Glaucoma is the leading cause of irreversible blindness in the world. Contrary to some conditions like cataract where patients get discharged after a successful surgery and sometimes never seen again, glaucoma is one of the areas of ophthalmology where you treat and follow up patients for life. I am a senior lecturer and consultant ophthalmologist at Ahmadu Bello University Teaching Hospital (ABUTH) in Nigeria and seeing a chance to help people in this difficult, life-changing journey I decided to contribute.
In my practice we see a number of people who are blind from glaucoma, and young individuals make a good proportion of these affected people. Accessibility and affordability play an important role in health care. This is more obvious in eye care and even more so in glaucoma. In the quest to provide affordable and accessible quality glaucoma care for people in low and middle income countries (LMICs), my research question was born.
In most LMICs, glaucoma diagnosis and management is done in secondary and tertiary centres where expertise and high-tech equipment are available. This causes a lot difficulties for people in rural areas to access such facilities. My PhD project is looking at the possibility of utilising community health centres in rendering glaucoma care through the use of portable and easy to use devices.
Our work is expected to demonstrate the use of portable devices in the detection of glaucoma, and that these devices could be comfortably used by community health workers to detect glaucoma and refer for further care. In the long run through earlier detection of this irreversible disease sight loss and blindness can be prevented. The success of this project will hopefully revolutionise glaucoma management in Nigeria and other LMICs, changing the narrative of blindness due to glaucoma.
I strongly think that public education and advocacy is important in glaucoma awareness. We need people also understand how it causes blindness and why early detection is significant in preventing blindness. We need governments and other institutions with an eye health mandate to also see the importance of preventing blindness due to glaucoma as an economic and public health concern.
Consideration should be given to glaucoma patients, especially in LMICs, by subsidising investigations and treatment. More support should be encouraged through research to come up with specific questions faced by eye health care professionals, in order to diagnosis and manage the different stages and types of glaucoma, thereby preventing blindness around the world.
Dr Farouk Garba is a senior lecturer and consultant ophthalmologist at Ahmadu Bello University Teaching Hospital (ABUTH), and also a pioneer ICO-World Glaucoma Association Fellow, 2017. He is presently undertaking his PhD at ICEH.
Dr. Southwood Smith was a great Victorian health reformer who became Minister for Health. “He was born in Mortock, in Somersetshire, began training to become a minister but his grant was withdrawn on the grounds that he was “entertaining opinions widely different from us on most of the doctrines we consider to be essential to Evangelical Religion”. “His family, which was narrowly religious, cast him off at once and for good. He married but his wife died young, leaving him at the age of 24 with two young children. In 1813 he decided to leave the children in the loving care of his wife’s relations and study medicine at Edinburgh University.
Passing his examinations in 1816, he married again, this time to a girl from Hackney, and came to London. He was appointed to The London Fever Hospital, then on the site of future King’s Cross Station. At this period, years before Pasteur, fever was a mysterious subject. Doctors could not distinguish one fever from the other. They still thought that disease was spread by smell (miasma) as the Greeks had done. It was before the realization that there were many forms of fever, with different causes. Bacterial infection was not understood. Everything was obscure. It would be generations before the different fevers were understood, and in the meantime, Southwood Smith’s thoughts were concentrated on how fevers in general might be prevented.
The Fever Hospital patients seemed to show a pattern. Patients (mainly women) came in with ‘a low fever’, were cured by rest and nursing, returned to their miserable homes, only to develop fever again. There seemed to be a connection between poor living conditions and ill-health. There was also some connection between being in the same house all day and going out to work somewhere else all day, as men did. He published reports on this.” https://www.locallocalhistory.co.uk/people/southwood-smith.htm
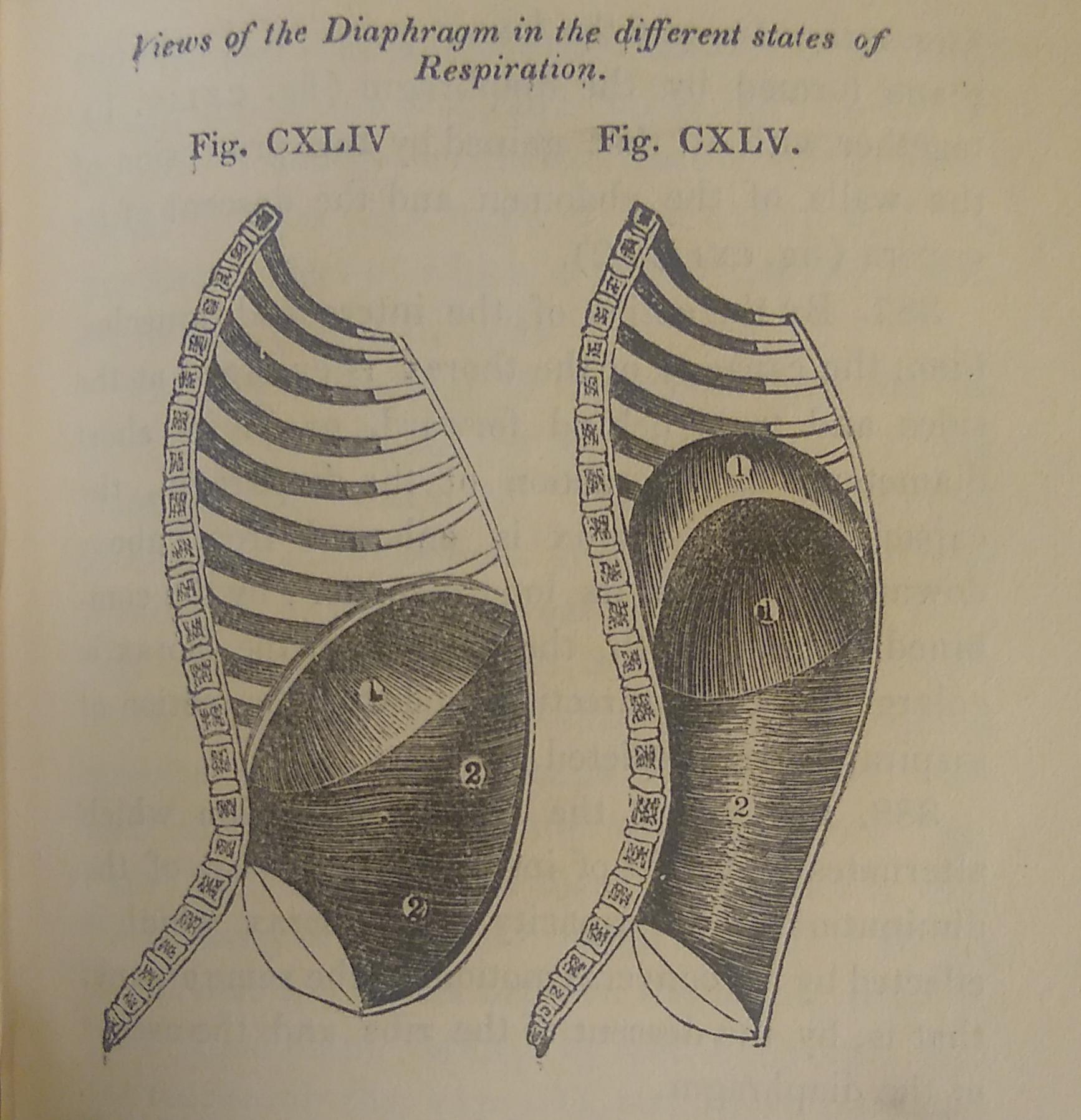
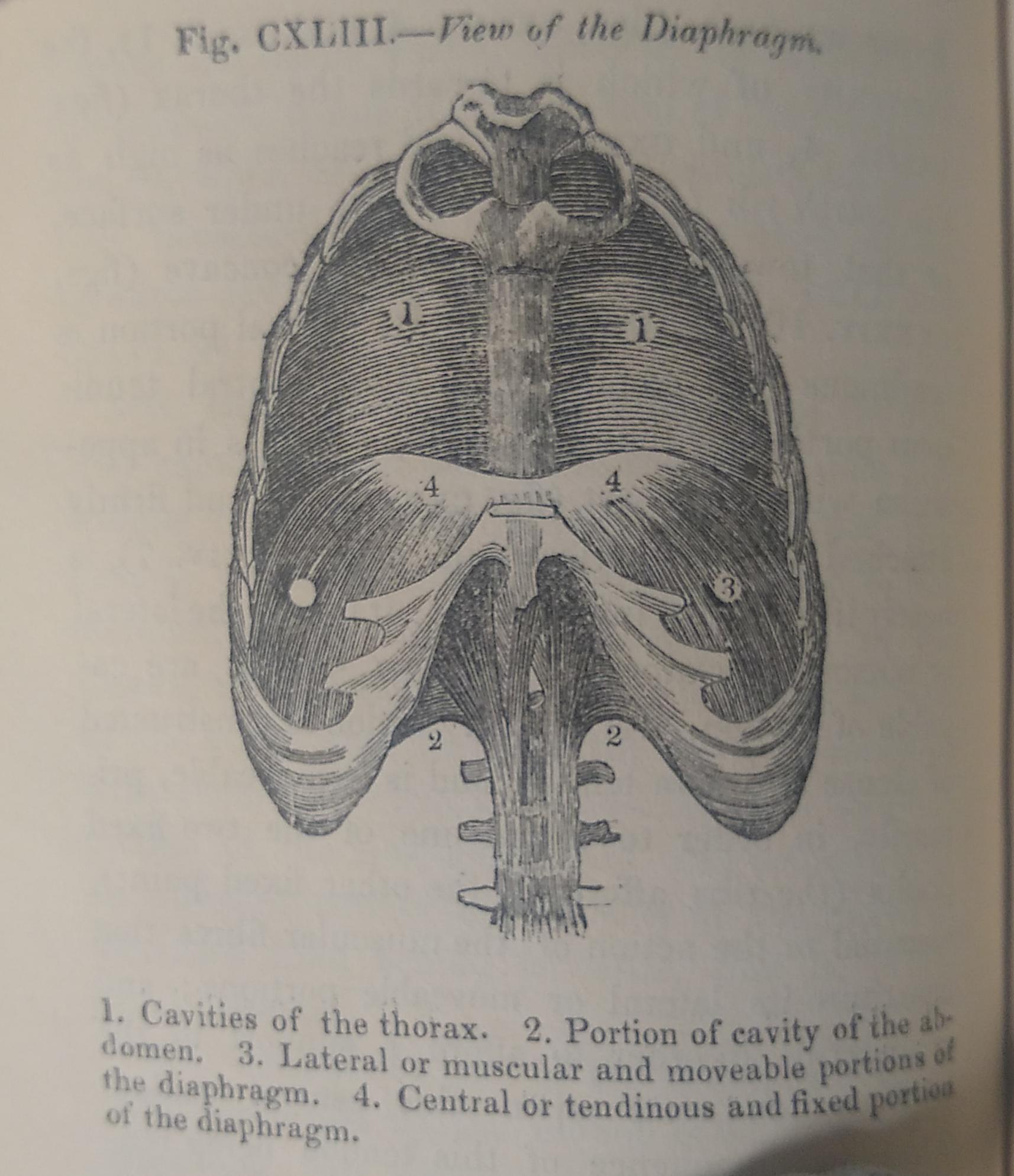
In Southwood Smith’s ‘ThePhilosophy of Health; an exposition of the physical and mental constitution of man with a view to the promotion of health and happiness’, he aims to give an account of the structure and functions of the body. Chapters on “respiration”, “the function of generating heat”, “the function of digestion”, “secretion”, “absorption” and “excretion” etc. are accompanied by philosophical musings and detailed drawings.
“Taking life in its most extended sense, as comprehending both the circles it includes, the organic and the animal (vol 1. Chap.2) it may be said to have three great centres, of which two relate to the organic, and the third to the animal life (vol 1. Chap. 2) The two systems which relate to the organic life are the systems of respiration and circulation; the third, which relates to the animal life is the nervous system. Of the organic life, the lungs and heart are the primary seats; of the animal, the brain and the spinal cord. Between each the bond of union is so close, that any lesion of the one influences the other, and neither can exist without the support of all. They form a triple chain, the breaking of a single link of which destroys the whole. (Vol II, p.113)
Reflecting on the interdependence of mind and body he observes “The mind is dependant on the body: hence an acquaintance with the physiology of the body should precede the study of the physiology of the mind. The constitution of the mind must be understood before its powers and affections can be properly developed and directed: hence a knowledge of the physiology of the mind is essential to a sound view of education and morals.” (Vol II, p.331)
His conviction that physical health depended on mental health foreshadows modern day concerns. “There is a close connexion between happiness and longevity. Enjoyment is not only the end of life, but it is the only condition of life which is compatible with a protracted term of existence. The happier a human being is, the longer he lives; the more he suffers, the sooner he dies; to add to enjoyment, is to lengthen life; to inflict pain is to shorten the duration of existence.” (Vol II, p.101)
Views of the Diaphragm in the different states of respiration p.59View of the Diaphragm p.58
Library users are welcome to consult any of these books on Library premises. To reserve a book for consultation, just go to their catalogue entry on Discover while you are logged into your LSHTM account and follow the instructions underneath the heading “Get It.” You’ll receive an email when it’s available. However, please note that these books will need to be read within the Library and cannot be borrowed like most other resources.
To mark International Women’s Day, I have put together a display of books authored or edited by a range of female staff and alumni of LSHTM. Among others there are Sari Kovats, Dina Balabanova, Virginia Berridge, Ann Mills and Anna Dixon. The topics include both the sciences and social sciences. Please do have a look next time you are in the Reading Room.
On a personal note, when I think of International Women’s Day I recall activities organized by the UCL UNISON* Women’s Group who brought such a wide range of issues to the branch as a whole, and in particular the late Wendy Biggin (picture, left) who would speak candidly about her experience of abusive relationships, and indeed showed great fortitude in resisting and overcoming institutional and cultural barriers. Wendy became involved in the union after the branch helped her to win back-pay while performing a more demanding work role. As an ally, branch member and personal friend I feel I learned a lot from her. Later on she was just about to set up her own counselling practice for women who had suffered domestic abuse when an aggressive breast cancer prevented her from doing so.
Today’s books from the LSHTM Historical Collection consist of some early attempts at gathering statistics on disease and society. Lots of the Collection significantly predates the foundation of LSHTM, which includes these volumes. Instead, the Library acquired them during the School’s early history, often through donations and bequests. This blogpost will take you through a few of the different ways books from the Collection presented data and findings, including tables, charts and maps.
Our edition of this book was published in 1750 in London. It contains tables from bills of mortality and parish registers. It also includes “observations” about how and why people might fall sick and die. Short also delves into a sort of epidemiology: he analyses the spread of epidemic disease in “sickly” years, seasonal diseases, and more.
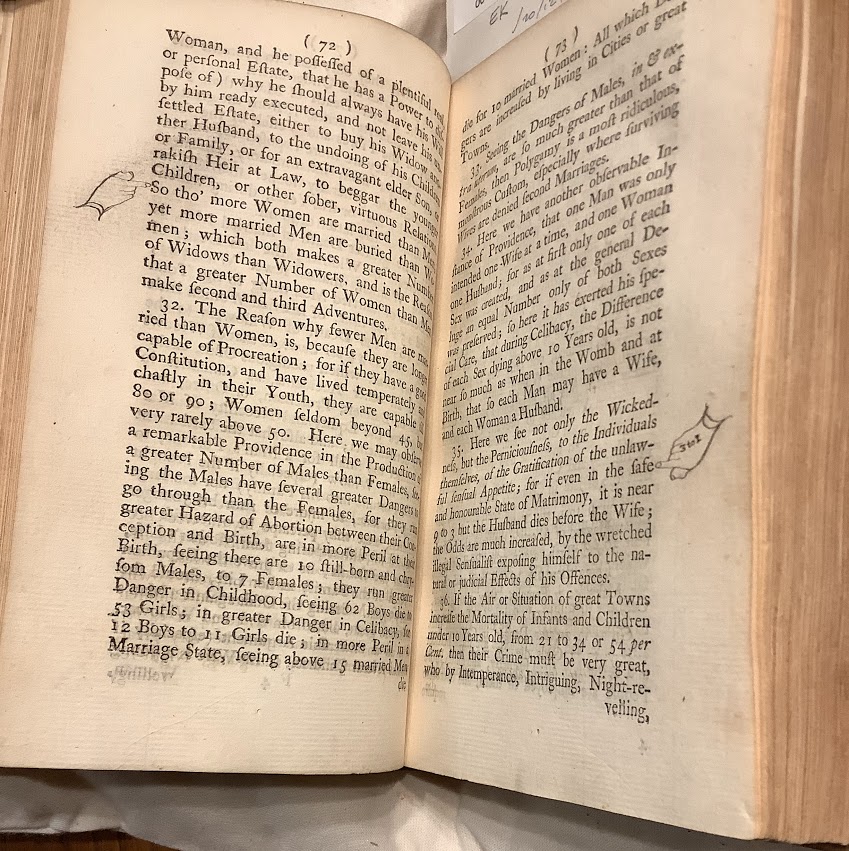
Yet Short frequently intersperses his number-crunching on births, marriages, and deaths with commentary on the nation’s morals and religion. For instance, activities Short especially opposed for health reasons included “Night Revelling,” “Passions,” and “theatrical Adventures and Intrigues.” (p.84). That suggests that Short saw strong links between contemporary behaviours and health. A past owner found his observations about marriage rates and morality (pp.72-3) especially interesting, adding pointing fingers to certain phrases – see below!
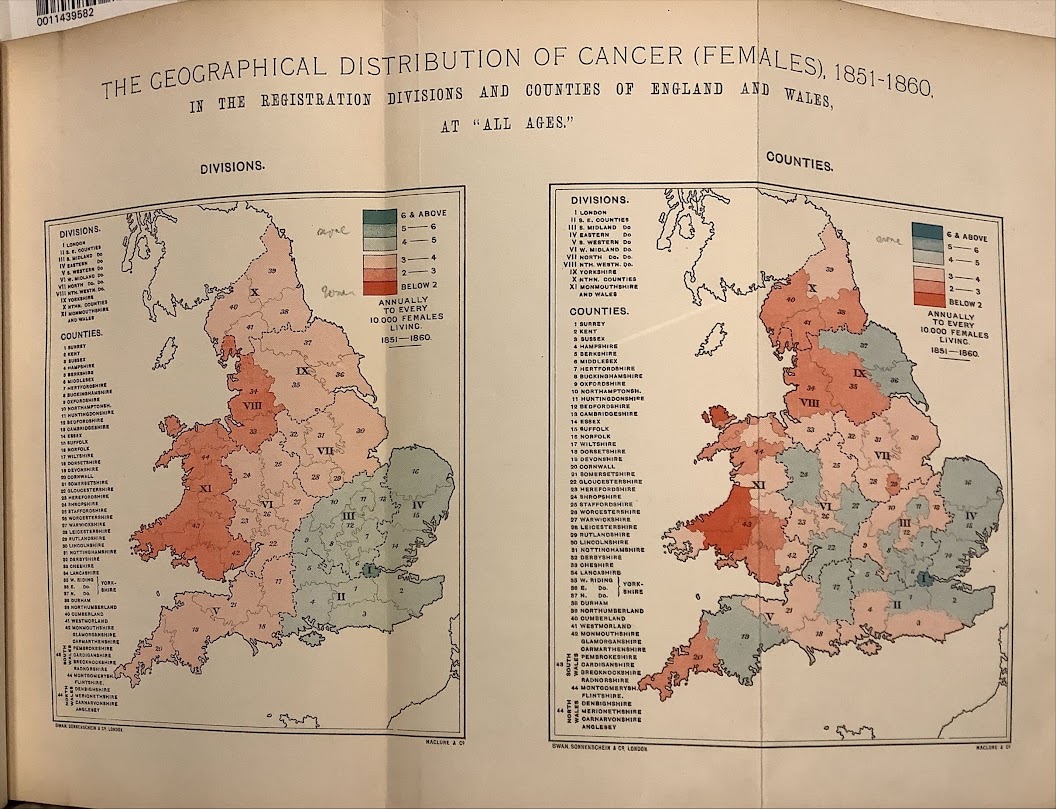
Sometimes statistics could be used to advance theories now known to be wrong. This is the case for this volume, written by Aldred Haviland. It contains some beautifully colourful maps in its attempts to advance the theory that geological phenomena caused cancers. For more on Haviland’s maps, see Frank A Barrett’s 1998 article. Additionally, he engages with theories circulated by contemporary anthropologists and ethnologists, primarily those of John Beddoe. Beddoe’s work, focusing on creating a typology of races in Britain and in particular categorising their hair or eye colour and skull measurements, means this geological-medical treatise can also be linked with the scientific racism of the time.
This volume offers a variety of statistics, from population numbers to education, wealth, crime, religious affiliations, and places of birth. Indeed, the public health section explores birth and death rates, along with statistics for various health facilities in the city. This included the Boston Medical Dispensary, an institution established in the late eighteenth century that was one of the first hospitals in the United States of America.
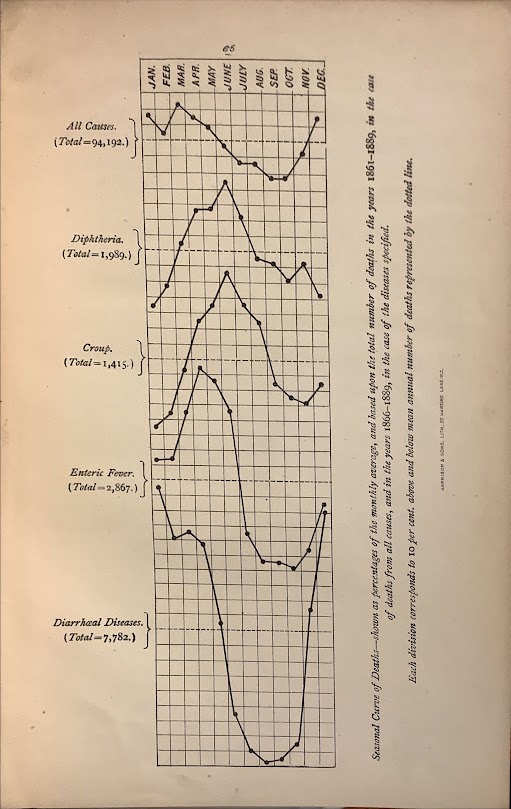
This volume, by T. Borthwick, was presented to the Library in the 1930s despite its 1891 publication date. It begins with south Australia’s geology and geography, proceeding to describe its population, including age distributions and country of birth, and birth-, marriage- and death-rates. It ends with a series of sections on different diseases, from malaria to diphtheria, and includes several charts at the very end.
The graph above, used to illustrate mortality and mortality from diseases during different months of the year, demonstrates how all-cause mortality but especially that from diarrheal diseases drops precipitously during the Australian winter months. It’s certainly a lot easier to read and to draw conclusions from than Short’s lengthy tables, with which we began.
Library users are welcome to consult any of these books on Library premises. To reserve a book for consultation, just go to their catalogue entry on Discover while you are logged into your LSHTM account and follow the instructions underneath the heading “Get It.” You’ll receive an email when it’s available. However, please note that these books will need to be read within the Library and cannot be borrowed like most other resources.
International Women’s Day (March 8) is a global day celebrating the social, economic, cultural and political achievements of women. Today is a great chance to remind ourselves of just some of the women who have studied and taught at LSHTM over the years.
Ida Kahn
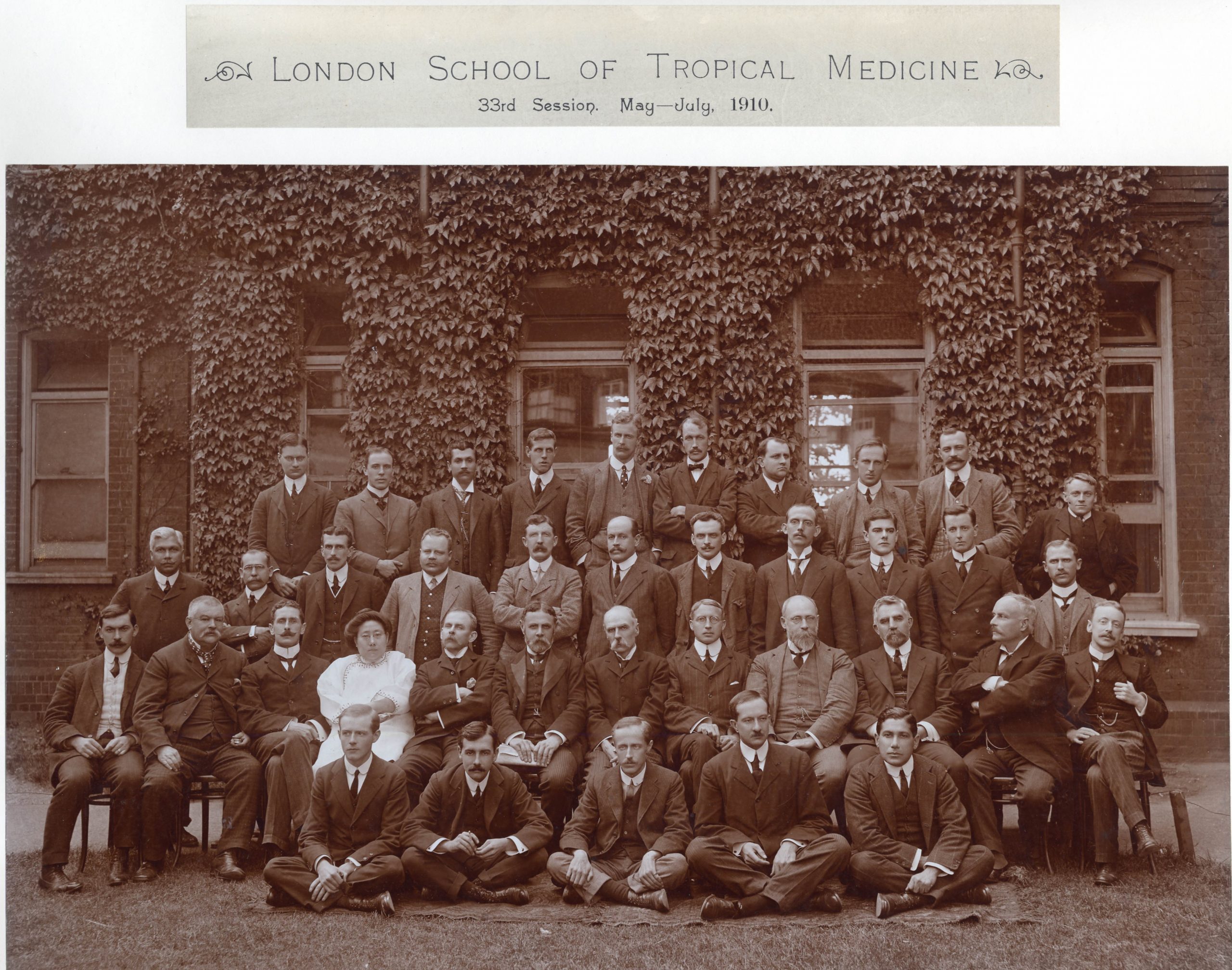
Group photograph of the 33rd Session (May-July 1910) at LSHTM. Ida Kahn is on the second row, fourth from the left.
Ida Kahn (born Kang Cheng) was the sixth girl in her family in Jiujiang, Jiangxi, China. She was adopted and renamed by her father’s employer, Gertude Howe. Raised as a Christian, her faith became a defining characteristic of her work. In her early life, Ida learned English and worked as a translator for foreign doctors.
In 1982, aged nineteen, she travelled to the United States to study for a degree in medicine from the University of Michigan. Ida was among the first Chinese women to become Western-trained physicians. Upon returning to Jiujiang in 1896 she worked as a medical missionary for the Women’s Foreign Missionary Society until her work was disrupted by the Boxer Rebellion.
Ida went back to the United States in 1908 to study literature at Northwestern University. She went on to study at the London School of Hygiene and Tropical Medicine between May-December 1910.
As one of the first Chinese women in the medical field, Ida worked to expand the presence of Chinese women in the workforce. Alongside Mary Stone, she established the first corps of Chinese women medical professionals. She was also influential in the building of the Nanchang Women and Children’s Hospital. She worked there until her death providing care to patients from all socioeconomic backgrounds.
Y.H. Hoa Shoo
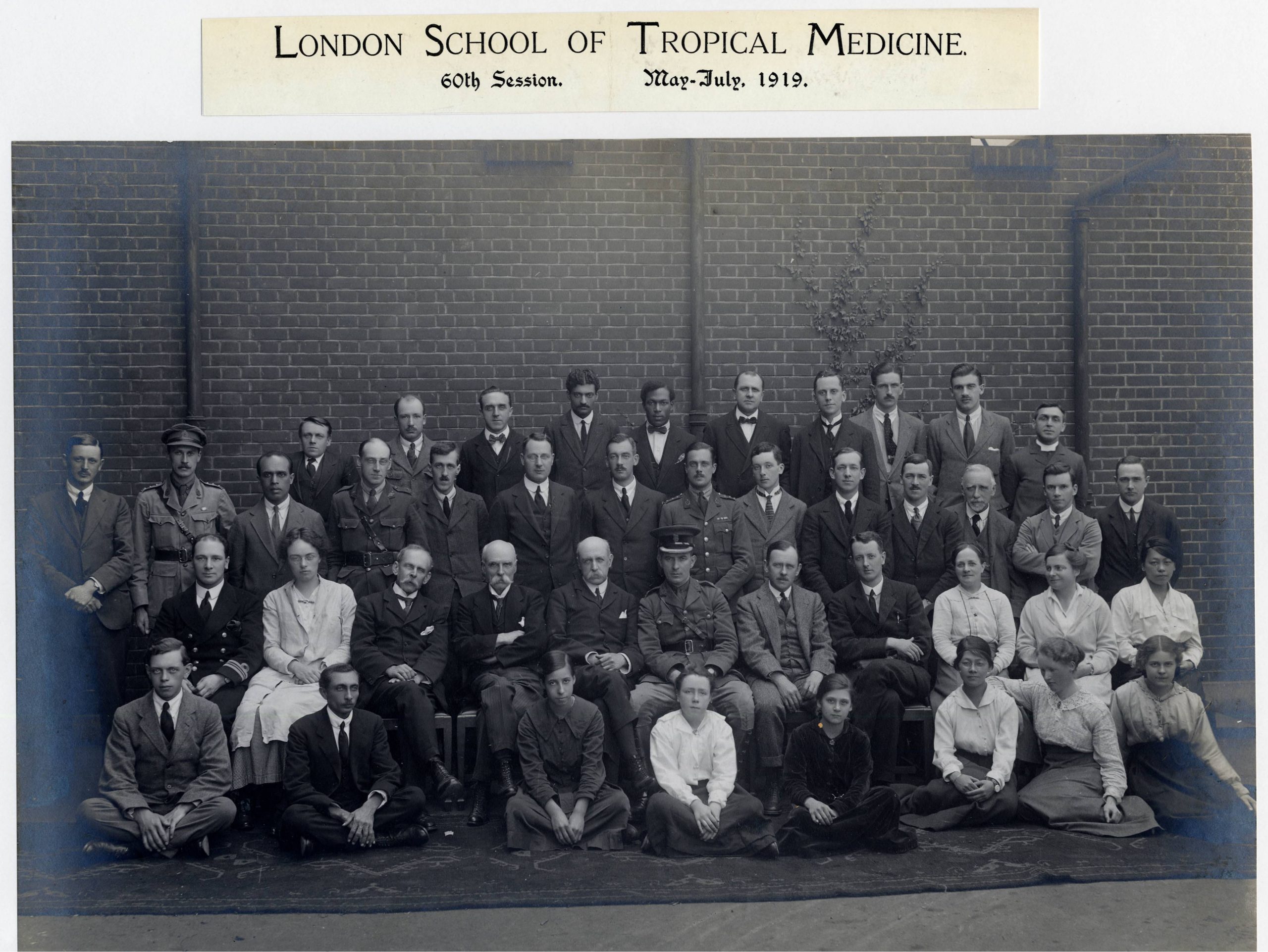
Group photograph of the 60th Session (May-July 1919) at LSHTM. Y.H. Hoa Shoo is on the second row, first on the right.
Dr Y.H. Hoa Shoo, attended LSHTM in 1919, where she passed the school’s exam with an impressive 70%. Prior to this, Hoa Shoo qualified in 1915 with a Bachelor of Medicine and a Bachelor of Human Biology.
After her studies at the School, Hoa Shoo returned to Singapore where she worked as a doctor in an Infant Welfare Centre in Penang, the centre that she would later run.
During the 1930s in Penang, infant mortality had steadily increased and became a concern to the local medical services. To combat this, an Infant Welfare Centre opened to provide mothers with education in infant feeding and care, and to monitor children’s health. By the late 1930s use of the clinics had gradually increased.
Little is known of Dr Hoa Shoo’s work in the Penang Infant Welfare Clinic. We do know that her career was cut short when she died on 5th October 1938, at the age of 45.
A.S. Gore and M.S. Gore
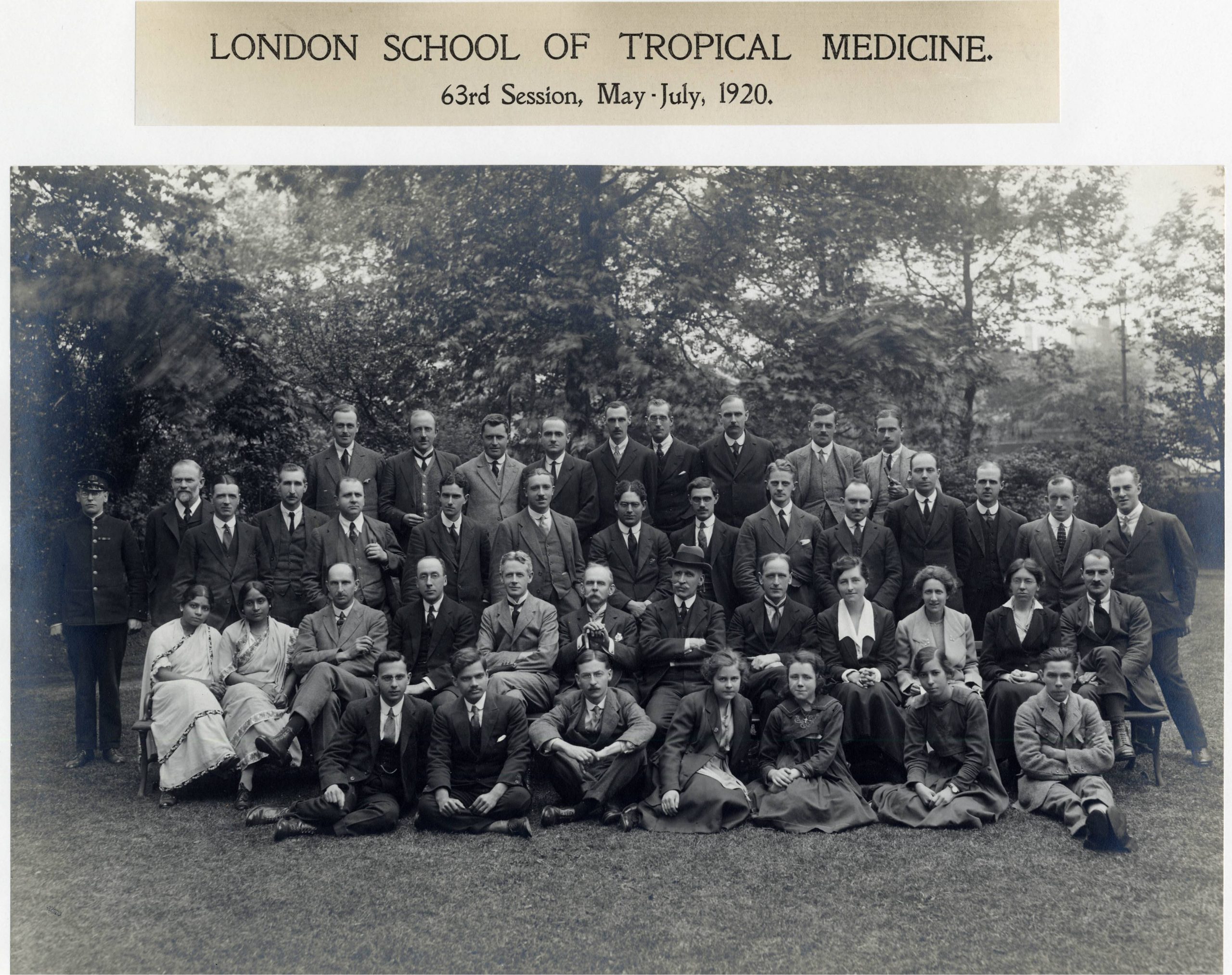
Group photograph of the 63rd Session (May-July 1920) at LSHTM. M.S. Gore (left) and A.S. Gore (right) are on the second row, first on the left.
Sisters, Miss A.S. Gore and Miss M.S. Gore were 24 and 23 when they attended LSHTM in 1920 to complete the School’s Diploma in Tropical Medicine. Both were already qualified in 1917 as Licentiate of the College of Physicians and Surgeons, a recognised medical qualification in India before 1946. They also attended a midwifery course in Dublin in 1920.
In India, during the later 19th and early 20th century, there was a great demand for female doctors, due in part, to the Indian government’s policy that medical services should be freely available to those employed in the manufacturing industries; an industry that employed many women. However many female students suffered from social pressure and few were able to complete their studies to qualify as a medical doctor.
The Gore sisters returned to India after completing the Diploma in Tropical Medicine course in 1920, but there is little information as to whether they continued to work in the medical profession.
Margot Jeffreys
Group photograph outside LSHTM’s Keppel Street building. Margot Jeffreys is on the first row, third from the left.
Margot Davies was born in Madras, India and studied history at the London School of Economics. During these years she met her future husband, James Jeffreys. She was a woman of principle, with deeply held beliefs in equality, liberty and justice.
Margot was appointed as lecturer in the Department of Public Health at the LSHTM in 1953. At the School, Margot taught medical sociology, and developed her research project on health and social services in Buckinghamshire.
During the 1960s Margot played an important part in establishing medical sociology as a distinct entity. In 1965 she became Director of Social Research and Senior Lecturer in Sociology at Bedford College. Here she worked to develop an internationally renowned Master’s programme.
Margot was also a consultant to the World Health Organization. She helped launch a research programme in the behavioural sciences and the sociology of medical education.
She engaged in research with the Royal Commission on Medical Education (1968), and the British Medical Association’s Working Group on Primary Health Care (1979), while maintaining her own research interests.
Margot retired in 1982, but continued with her research in retirement. The late 1980s saw a resurgence of interest in social science and medical sociology at LSHTM.
Jennifer Roberts
Dr Jenny Roberts was a pioneer of Health Economics, becoming the first Health Economist at the School. Born into a mining family in North Wales, she won a miners’ scholarship to the London School of Economics aged 21.
In 1972 the Centre for Extension Training in Community Medicine was established. Its aim was to provide specialist training for public health and community medicine personnel involved in the first major re-organisation of the National Health Service. Jenny provided the economic input. The Centre was amalgamated with LSHTM’s Department of Community Health in 1976. Jenny was the first economist to be employed by the School. She played a key role in establishing health economics as an internationally important field.
With Brian Abel-Smith, she set up a new MSc in Health Policy, Planning and Financing. This course ensured the establishment and expansion of the discipline of health economics at the LSHTM and internationally.
In the 1980s, Jenny researched the market-based NHS reforms. She looked at the links between the use of contracted-out NHS services, and the increase in Hospital Acquired Infections. Jenny’s extensive research into the economic costs of diseases including HIV/AIDS, resurgent tuberculosis, new gastro-enteric, and hospital-acquired infections, revealed the economic burden, both for providers of health care, and for those affected by these diseases.
Jenny’s last major publication, The Economics of Infectious Disease (Oxford, 2008) is a testament to the importance of her discipline in the management and control of the world’s on-going problems of infectious disease.
LSHTM Archives holds her collection and you can explore it here.
Bascombe’s ‘A History of Epidemic Pestilences from the earliest ages 1495 years before the birth of our Saviour to 1848’, is a historical account of diseases around the world. Since there was no concept of germ theory, no one understood the cause of these outbreaks or how they spread and so they were often attributed to supernatural causes. In his book these occurrences of ‘pestilence’ often coincide with comets. In AD 1401 “A comet was seen. Pestilence broke out at Florence. 30,000 persons died of epidemic disease this year in London”. (p. 38) The year 1819 “was marked by great commotions of the elements, and a general spread of epidemic pestilence all over the world. “(p.153)
The symptoms ascribed to these ‘pestilences’ are sometimes quite extraordinary and seem to suggest a kind of mass hysteria.
In AD 1374 “the epidemic dancing disease of St. Guy and St. John prevailed in Holland and in the Renish provinces …The disease also prevailed in France and the sufferers were called ‘Convulsionnaires;’…Hecker gives the following account of this strange malady..it was a convulsion which, in the most extraordinary manner, infuriated the human frame, and excited the astonishment of contemporaries for more than two centuries..It was called the Dance of St John or of St Victus, on account of the Bacchantic leaps by which it is characterized, and which gave to those affected , whilst performing their wild dance, and screaming and foaming with fury, all the appearance of persons possessed…(p.56) They formed circles hand-in-hand and, appearing to have lost all control over their senses, continued dancing, regardless of the bystanders for hours together, in wild delirium, until at length they fell down to the ground in a state of exhaustion.” (p.57)
In AD418 “Strasburgh was visited by the ‘Dancing Plague’ and the same infatuation existed amongst the people there as in the towns of Belgium and the Lower Rhine AD 1374; many who were seized on seeing the affected, excited attention at first by their confused and absurd behaviour, and then by their constantly following the swarms of dancers. These were seen day and night passing through the streets , accompanied by musicians playing on bagpipes, and by innumerable spectators attracted by curiosity, “(p. 63)
There were numerous plagues alongside more mysterious illnesses such as the ‘sweating sickness’, which made its appearance in England in A.D.1517. “So rapid and violent was this disease in its course, that it carried off those who were attacked in two of three hours, so that the first shivering fit was the announcement of death; many who were in good health at noon-day were corpses by evening.” (p. 77)
Library users are welcome to consult any of these books on Library premises. To reserve a book, just go to the catalogue entry on Discover while you are logged into your LSHTM account and follow the instructions underneath the heading “Get It.” You’ll receive an email when it’s available. However, please note that these books will need to be read within the Library and cannot be borrowed like other resources.
Cataract is the leading cause of blindness globally, and a major cause of vision impairment, affecting an estimated 94 million people in 2020. The scale of this challenge is not spread equally however, with some places and population groups experiencing much higher prevalence of the potentially blinding condition, despite surgery being a highly cost-effective treatment.
A new global study led by the International Centre for Eye Health has identified the groups most underserved by cataract services in different world regions, as well as the most promising strategies to improve access of these groups. This information is useful as countries respond to the ambitious global target set by member states at the 74th World Health Assembly to increase effective cataract surgical coverage (ecsc) by 30 percentage points by 2030. Ecsc is a measure of how many people with cataract needing surgery have received it with a good outcome.
The study used a Delphi process, a widely used expert consultation method, to identify and prioritise underserved groups and promising strategies. The process included 183 panellists who are knowledgeable about cataract services. The panel was made up of 46% women and included representatives from all seven Global Burden of Disease (GBD) Super Regions.
Panel members were asked which groups in their setting experienced the most difficulty accessing cataract services, followed by what interventions in their area are most effective at increasing their access to both screening and surgical services. Panellists were encouraged to include as many opinions as possible to maximise the chance of identifying the most important ideas.
Following a prioritisation process, at the global level the groups ranked highest in terms of being a large group and having the most difficulty accessing services were rural/remote dwellers, people with low socioeconomic status and people with low social support. Other groups which were considered to be smaller than these three but having the most difficulty with access were people without housing and people with disabilities. Despite evidence showing that women have lower access to cataract services in most world regions, panellists tended not to identify women as an underserved group.
In terms of strategies to improve access to screening services, the study group considered the most promising strategies to be policy development for primary care screening programmes and strengthening the skills of primary care staff. Further strategies included establishing permanent services closer to the community level and eliminating the out-of-pocket costs for patients that need care. Potential solutions for reducing costs, which can prevent people from travelling to or paying for the care they need, were free screening, including screening within insurance coverage and providing transport.
Panellists thought access to surgical services could be improved by decentralizing services so that surgery was permanently available at the district level or below. Strengthening integration between screening, referral, surgery and follow-up, reducing out-of-pocket costs for surgery and post-operative care, providing universal health insurance that includes cataract surgery and delivering good quality outcomes were also prioritised as good strategies.
This is believed to be the first study to attempt these specific questions, and the answers highlight the need for context-specific approaches to improve access to cataract services and promote equity.
Recommendations from the study that can be considered by governments and their partners in pursuit of improvements in ecsc include:
Supporting health information systems to strengthen monitoring of inequality and provide evidence for policy and planning
Including the intersection of gender with other social attributes in future research to consider the disproportionate disadvantage experienced by some women
When planning services, each global region can refer to the list developed in this research for the activities most promising and feasible in their setting. The study can serve as a ‘menu of strategies’ that can be tested, alone or in combination with others to improve services within an area.
The authors believe these results can serve eye health decision-makers, researchers and funders as a starting point for coordinated action to improve access to cataract services, particularly among population groups who have historically been left behind.
Publication: Ramke J, Silva JC, Gichangi M, The Cataract Access Study Group, et al. Cataract services for all: strategies for equitable access from a global modified Delphi process. PLOS Global Public Health. February 2022. https://doi.org/10.1371/journal.pgph.0000631
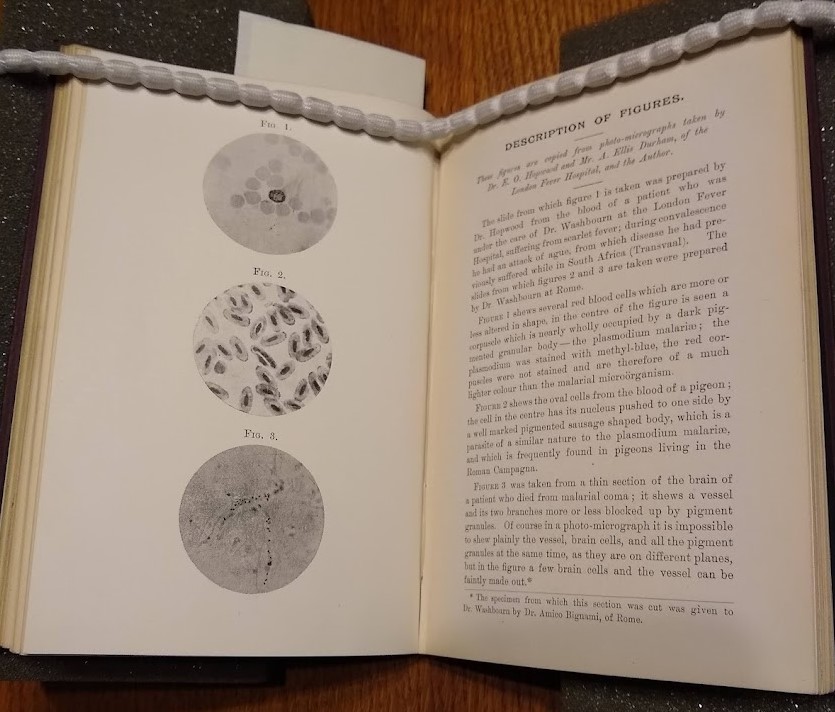
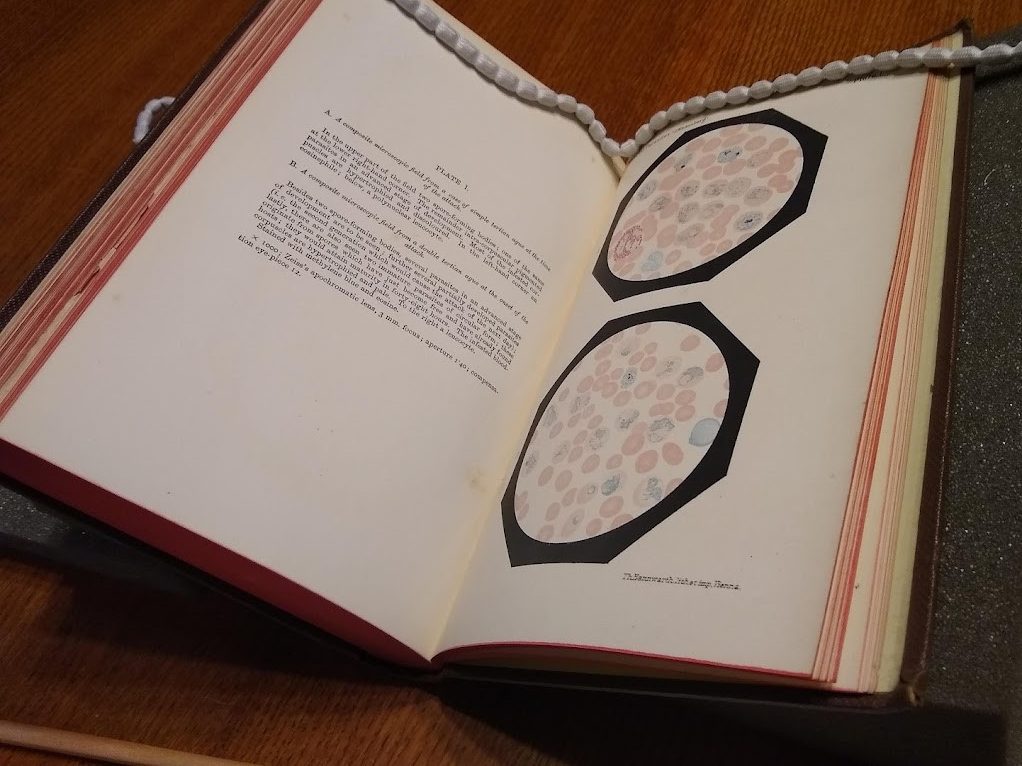
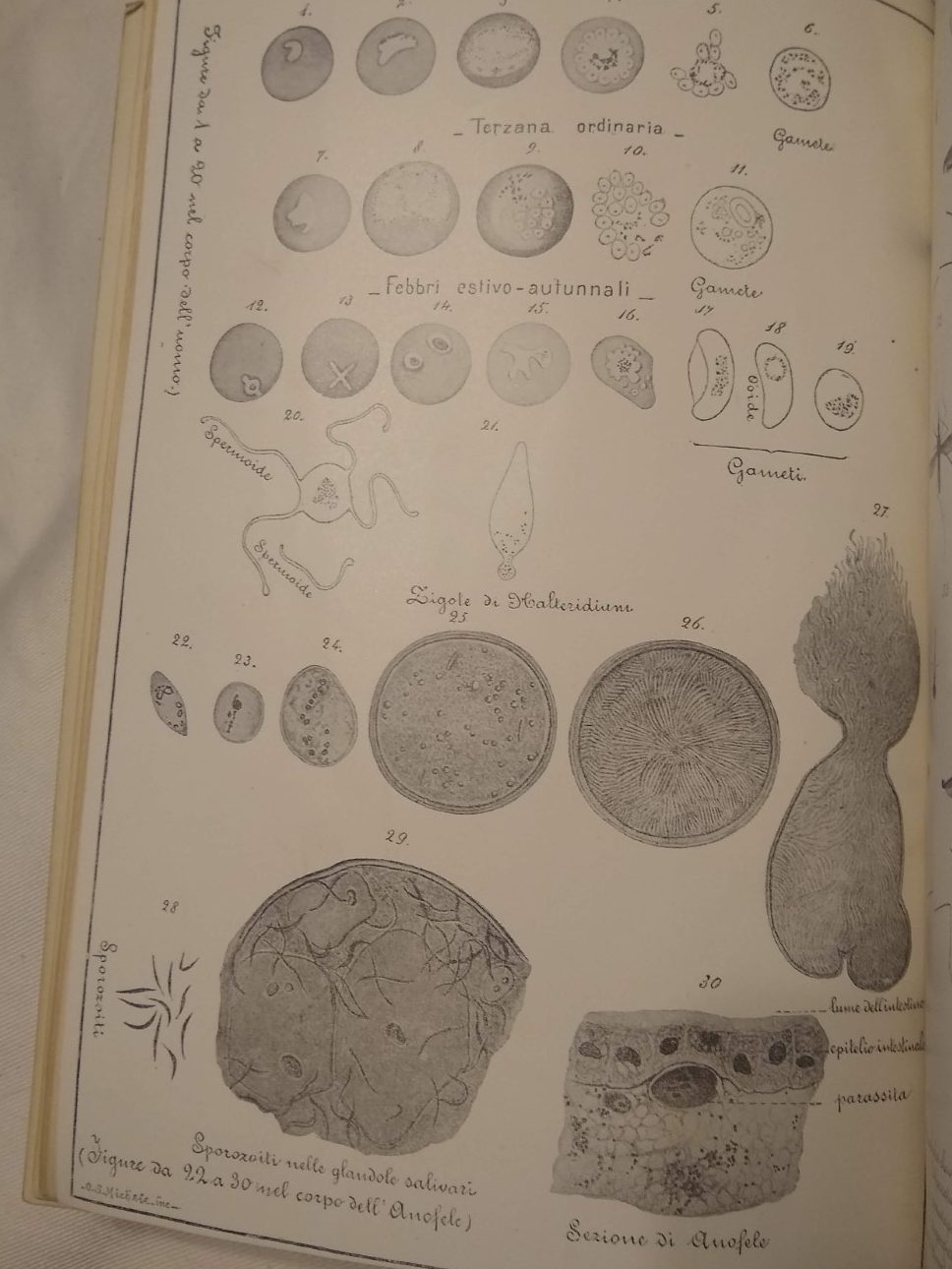
As shown in the recent report on LSHTM’s colonial history, the financial burden of malaria on the British colonial project was one of the driving forces behind the LSTM’s foundation. It’s therefore unsurprising to find that many books on malaria are in the Historical Collection. Many of them contain detailed illustrations of the Plasmodium parasite and its effect on red blood cells, while offering colourful explanations of how their authors thought it worked while doctors gradually established the disease’s mechanisms and modes of transmission.
The Collections team at LSHTM Library has been hard at work on improving the catalogue records for the Historical Collection. Overall, this Collection consists of many of our older volumes, which have often been in the possession of the Institute for decades, if not over a century. While few offer up-to-date information on the medical or social sciences, these books are valuable sources on the history of medicine at LSHTM and beyond.
Books containing outdated and offensive language have been marked as ‘culturally sensitive’ e.g., Roman Fever, plate pictured above, or Malaria: what it means and how avoided.
Additionally, the improved metadata includes details of the book’s binding, describing the colour, endpapers, materials, and so on. This can also include details on the book’s provenance like bookplates.
Many of these books are also accessible online on the Internet Archive thanks to a project in 2015 which digitised them for the UK Medical Heritage Library. Moreover, links to digitised copies are available on the library catalogue entries for the books.
Library users are welcome to consult any of these books on Library premises. To reserve a book, just go to their catalogue entry on Discover while you are logged into your LSHTM account and follow the instructions underneath the heading “Get It.” You’ll receive an email when it’s available. However, please note that these books will need to be read within the Library and cannot be borrowed like other resources.
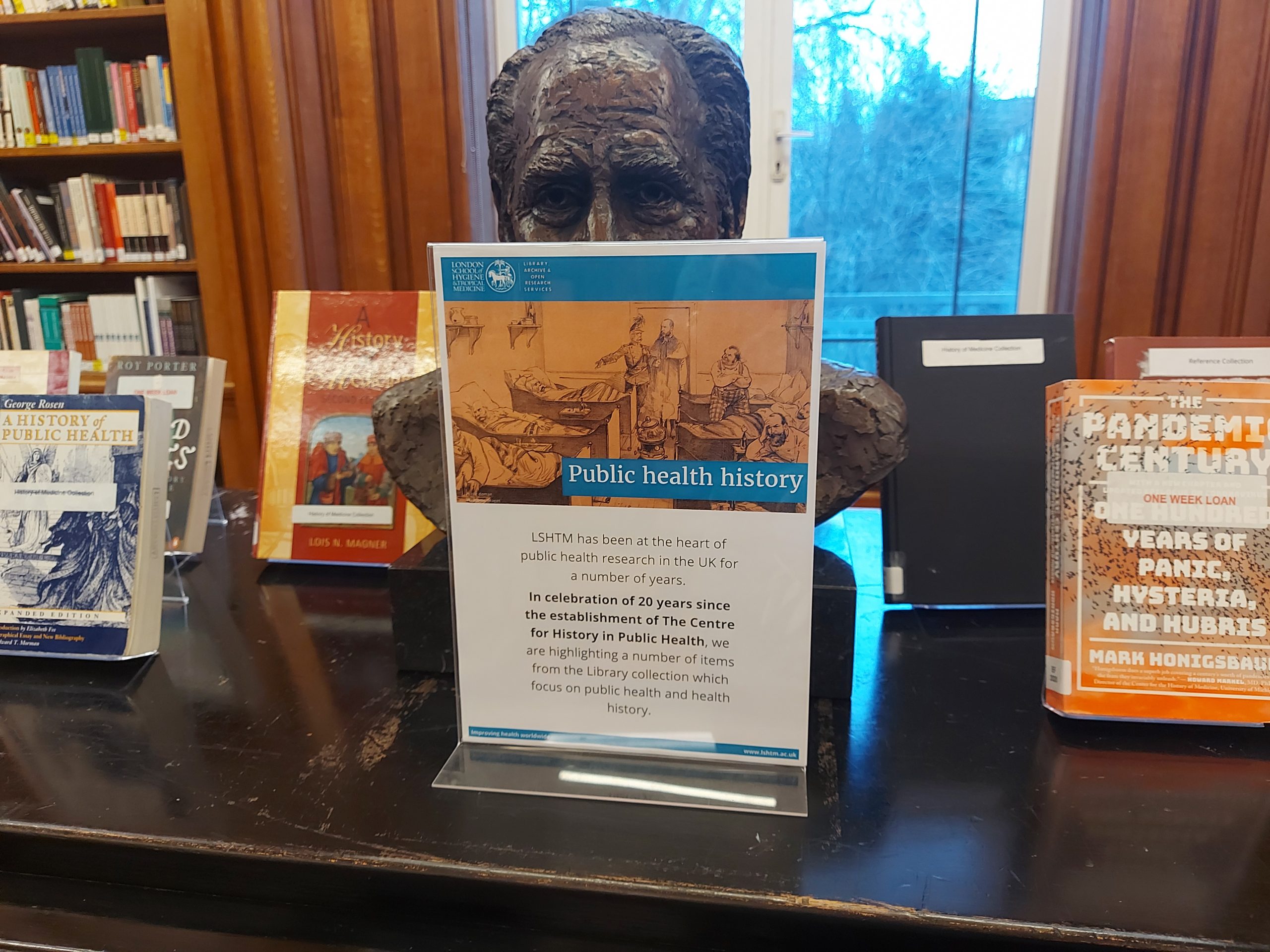
The Library is celebrating twenty years of the Centre for History in Public Health with a book display, highlighting a number of items in the library collection which focus on subjects around health history and public health history.
The Centre was formed in 2003, but has its origins in late 1980s, initially forming as the AIDS Social History Programme and then expanding into other areas of public health history during the 1990s. The Centre is at the forefront of public health history research in the UK.
“Historical research is of central relevance to an understanding of public health in the present. Current developments cannot be understood without a knowledge of the past.” (CHiPH website).
The library is highlighting a number of books around public health and health history, in celebration of 20 years of the Centre for History in Public Health.
The Centre’s research largely focuses on 20th and 21st century history, and has been involved with a lot of research in the area including HIV, Covid, charity and smoking. More information can be found here: https://www.lshtm.ac.uk/research/centres/centre-history-public-health/publications. It is also important to highlight the great outreach work the Centre is involved with, to help educate the public and improve awareness of issues. Including exhibitions, walks and film screenings.
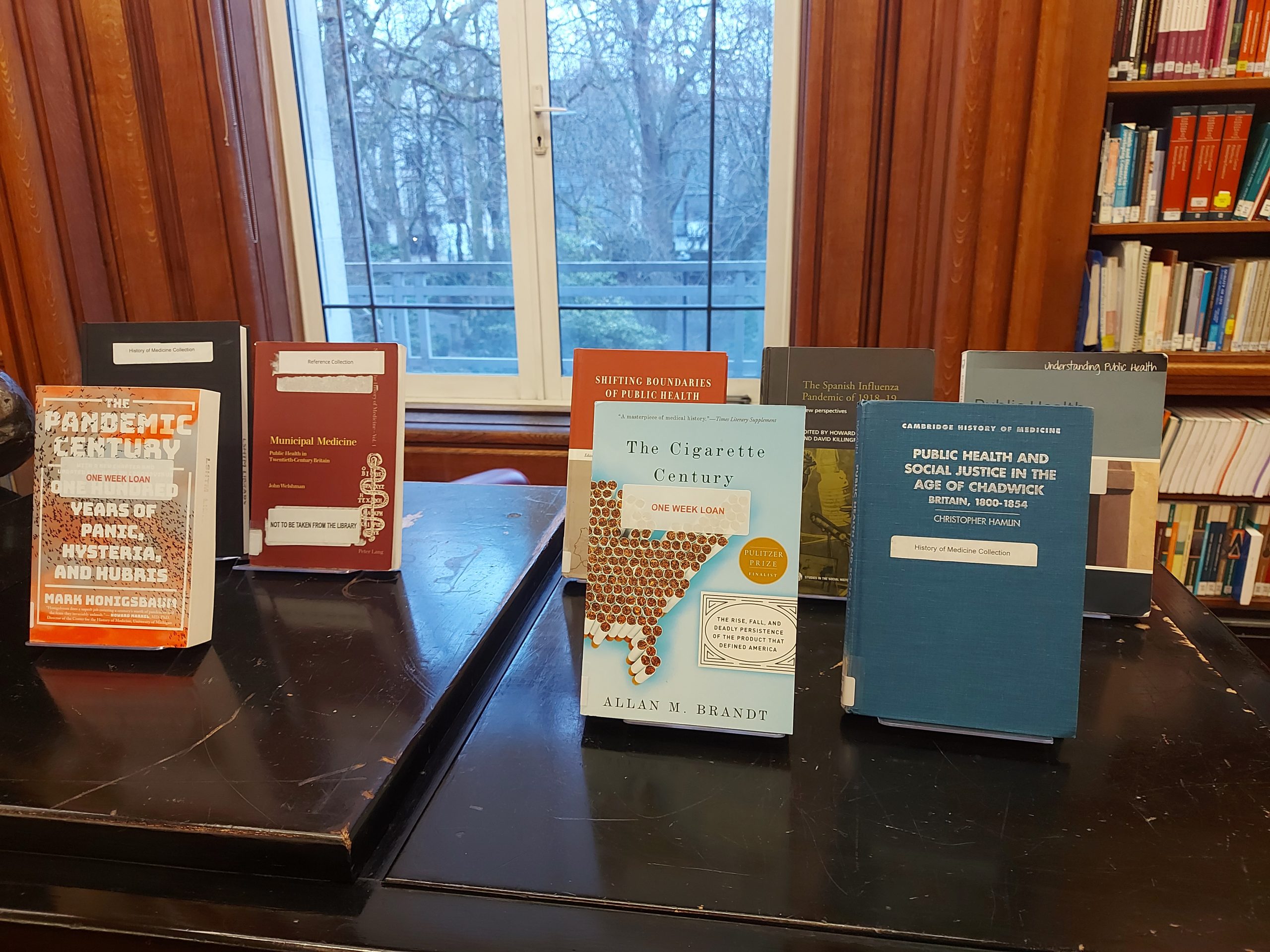
Hopefully a book on display may peak your interest, they can all be loaned out by students, staff and library members and here’s to the next twenty years of the Centre for History in Public Health.
A few of the books on display currently in the library, celebrating public health history.
More books and other items in and around the topic of public health history can be found under several shelf marks: SO.D (Public Health History), D (History of Medicine) and you may also find items under more specialist areas GFW (smoking, tobacco etc), KM (AIDS/HIV).
Around 500 million people worldwide suffer from untreated near-vision impairment, which can impair people’s ability to live and work. ICEH’s close partner Peek Vision, which works to create tools to improve eye care, has now completed validation of a smartphone-based near vision test.
A study carried out by Peek Vision, ICEH and Nepal Netra Jyoti Sangh, the largest eye care provider in Nepal, compared the Peek Near Vision Test to a conventional chart used for vision testing. The findings showed that the near vision test is valid for identifying people with near visual impairment and as a quantitative assessment of the score of near visual acuity.
Peek Vision has been using a validated distance vision test for nearly a decade, which is used across their programmes worldwide. The next steps for the near vision test will be incorporation into tools and programmes, and for population data studies.
Additional results from the study found high levels of repeatability among independent examiners, further proving the accuracy and reliability of this test.
Lead Researcher and Peek team member, Dr Marzieh Katibeh, said on the benefits of the study:
“The original Peek Acuity app, which tests distance vision only, has been successfully validated and embedded across numerous programmes worldwide. Combining this with digital near vision testing, particularly in populations at risk of presbyopia who can be identified in the same visit, will facilitate the identification and management of both near and distance visual impairments. It may also make vision measurement more appealing to organisers of community health surveys and surveillance who are already using digital devices for data collection. The Peek Near Vision test we have validated in this study could serve this purpose.”